

Heart failure with recovered ejection fraction: clinical description, biomarkers, and outcomes
- PMID: 24799515
- PMCID: PMC4053508
- DOI: 10.1161/CIRCULATIONAHA.113.006855
Heart failure with recovered ejection fraction: clinical description, biomarkers, and outcomes
Abstract
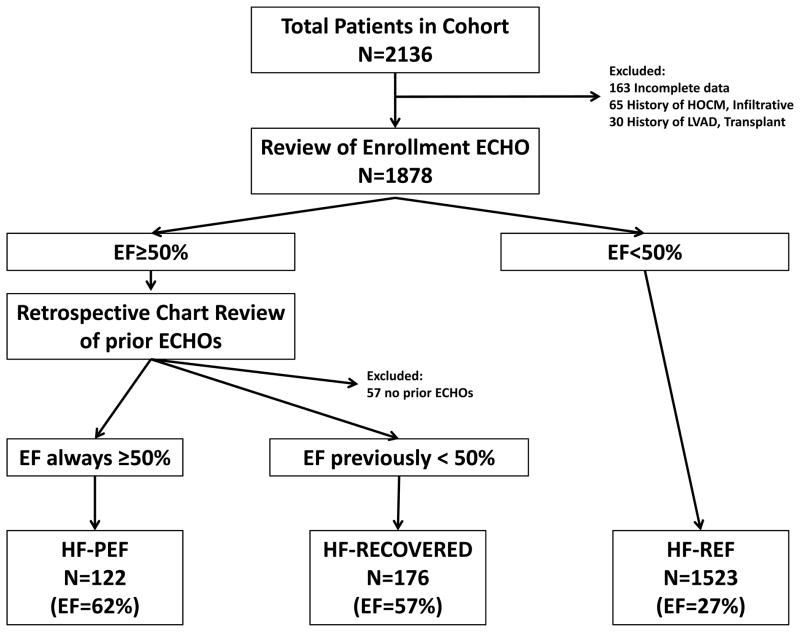
Background: We hypothesized that patients with heart failure (HF) who recover left ventricular function (HF-Recovered) have a distinct clinical phenotype, biology, and prognosis compared with patients with HF with reduced ejection fraction (HF-REF) and those with HF with preserved ejection fraction (HF-PEF).
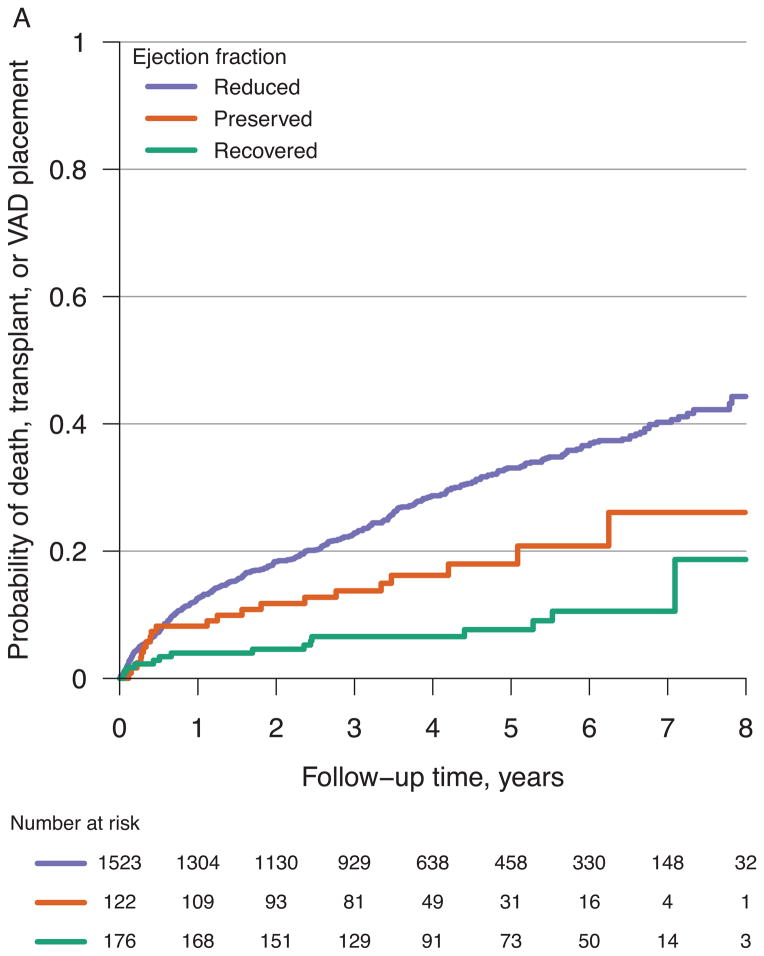
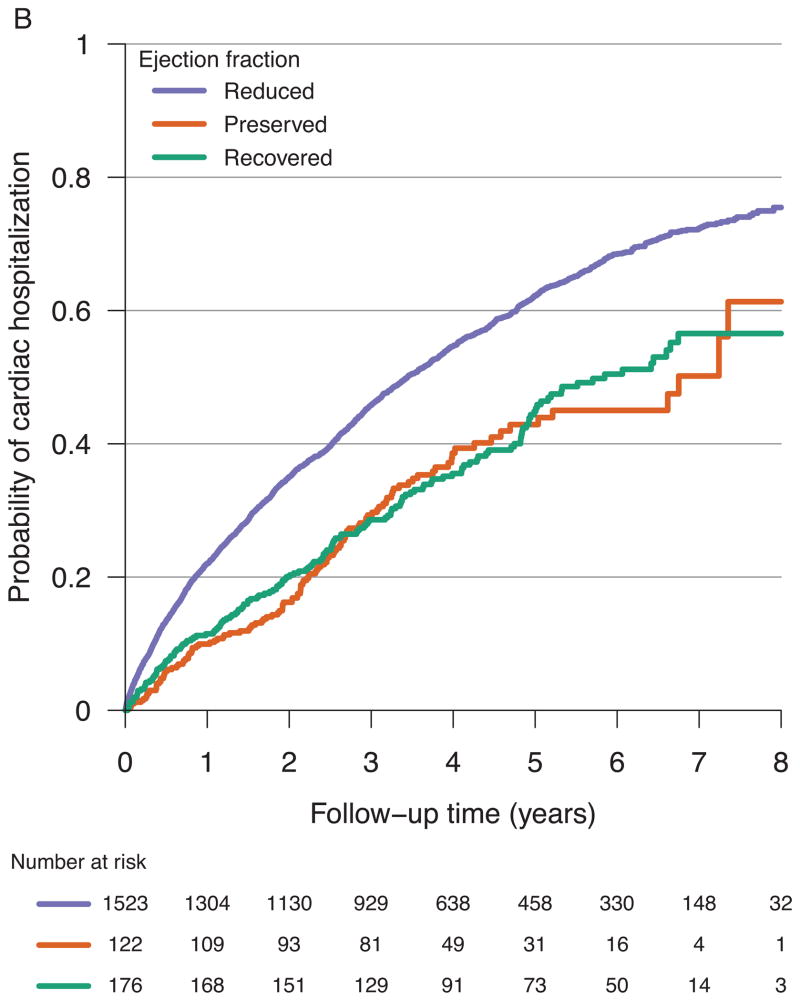
Methods and results: The Penn Heart Failure Study (PHFS) is a prospective cohort of 1821 chronic HF patients recruited from tertiary HF clinics. Participants were divided into 3 categories based on echocardiograms: HF-REF if EF was <50%, HF-PEF if EF was consistently ≥50%, and HF-Recovered if EF on enrollment in PHFS was ≥50% but prior EF was <50%. A significant portion of HF-Recovered patients had an abnormal biomarker profile at baseline, including 44% with detectable troponin I, although in comparison, median levels of brain natriuretic factor, soluble fms-like tyrosine kinase receptor-1, troponin I, and creatinine were greater in HF-REF and HF-PEF patients. In unadjusted Cox models over a maximum follow-up of 8.9 years, the hazard ratio for death, transplantation, or ventricular assist device placement in HF-REF patients was 4.1 (95% confidence interval, 2.4-6.8; P<0.001) and in HF-PEF patients was 2.3 (95% confidence interval, 1.2-4.5; P=0.013) compared with HF-Recovered patients. The unadjusted hazard ratio for cardiac hospitalization in HF-REF patients was 2.0 (95% confidence interval, 1.5-2.7; P<0.001) and in HF-PEF patients was 1.3 (95% confidence interval, 0.90-2.0; P=0.15) compared with HF-Recovered patients. Results were similar in adjusted models.
Conclusions: HF-Recovered is associated with a better biomarker profile and event-free survival than HF-REF and HF-PEF. However, these patients still have abnormalities in biomarkers and experience a significant number of HF hospitalizations, suggesting persistent HF risk.
Keywords: heart failure; myocardium; ventricular remodeling.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Figures
Comment in
-
Heart failure with better ejection fraction: a modern diagnosis.Circulation. 2014 Jun 10;129(23):2364-7. doi: 10.1161/CIRCULATIONAHA.114.010194. Epub 2014 May 5. Circulation. 2014. PMID: 24799514 No abstract available.
-
Letter by Psaty et al regarding article, "Heart failure with recovered ejection fraction: clinical description, biomarkers, and outcomes".Circulation. 2015 Feb 10;131(6):e343. doi: 10.1161/circulationaha.114.012243. Circulation. 2015. PMID: 25815392 No abstract available.
-
Response to letter regarding article, "Heart failure with recovered ejection fraction: clinical description, biomarkers, and outcomes".Circulation. 2015 Feb 10;131(6):e344. doi: 10.1161/circulationaha.114.012888. Circulation. 2015. PMID: 25815393 No abstract available.
References
-
- Konstam MA, Rousseau MF, Kronenberg MW, Udelson JE, Melin J, Stewart D, Dolan N, Edens TR, Ahn S, Kinan D. Effects of the angiotensin converting enzyme inhibitor enalapril on the long-term progression of left ventricular dysfunction in patients with heart failure. SOLVD Investigators. Circulation. 1992;86:431–8. - PubMed
-
- Packer M, Colucci WS, Sackner-Bernstein JD, Liang CS, Goldscher DA, Freeman I, Kukin ML, Kinhal V, Udelson JE, Klapholz M, Gottlieb SS, Pearle D, Cody RJ, Gregory JJ, Kantrowitz NE, LeJemtel TH, Young ST, Lukas MA, Shusterman NH for the PRECISE Study Group. Double-blind placebo-controlled study of the effects of carvedilol in patients with moderate to severe heart failure. The PRECISE trial. Prospective Randomized Evaluation of Carvedilol on Symptoms and Exercise. Circulation. 1996;94:2793–9. - PubMed
-
- Sutton MG, Plappert T, Abraham WT, Smith AL, DeLurgio DB, Leon AR, Loh E, Kocovic DZ, Fisher WG, Ellestad M, Messenger J, Kruger K, Hilpisch KE, Hill MR Multicenter InSync Randomized Clinical Evaluation (MIRACLE) Study Group. Effect of cardiac resynchronization therapy on left ventricular size and function in chronic heart failure. Circulation. 2003;107:1985–90. - PubMed
-
- Bax JJ, Poldermans D, Elhendy A, Cornel JH, Boersma E, Rambaldi R, Roelandt JR, Fioretti PM. Improvement of left ventricular ejection fraction, heart failure symptoms and prognosis after revascularization in patients with chronic coronary artery disease and viable myocardium detected by dobutamine stress echocardiography. J Am Coll Cardiol. 1999;34:163–169. - PubMed
-
- Boehmer JP, Starling RC, Cooper LT, Torre-Amione G, Wittstein I, Dec GW, Markham DW, Zucker MJ, Gorcsan J, 3rd, McTiernan C, Kip K, McNamara DM IMAC Investigators. Left ventricular assist device support and myocardial recovery in recent onset cardiomyopathy. J Card Fail. 2012;18:755–61. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
