

Nuclear medicine dynamic investigations in the diagnosis of Budd-Chiari syndrome
- PMID: 24799994
- PMCID: PMC4009481
- DOI: 10.4254/wjh.v6.i4.251
Nuclear medicine dynamic investigations in the diagnosis of Budd-Chiari syndrome
Abstract
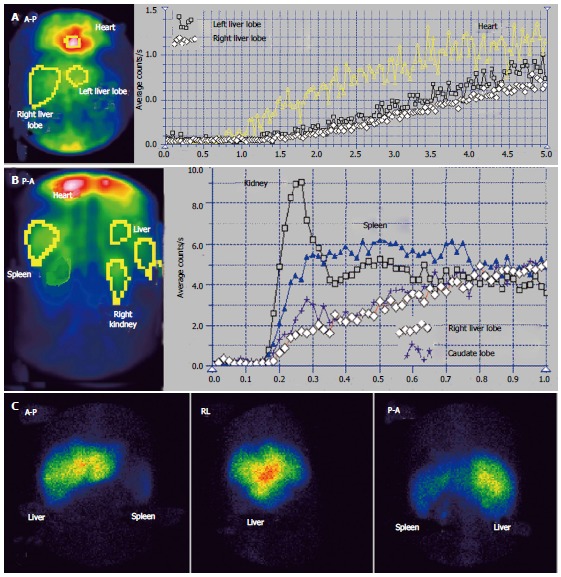
Aim: To investigate the hepatic hemodynamics in the Budd-Chiari syndrome (BCS) using per-rectal portal scintigraphy (PRPS) and liver angioscintigraphy (LAS).
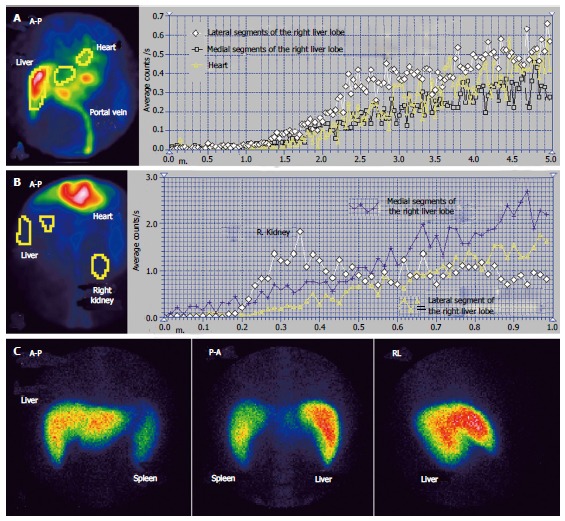
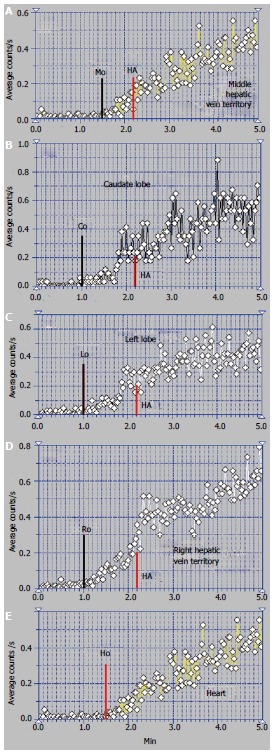
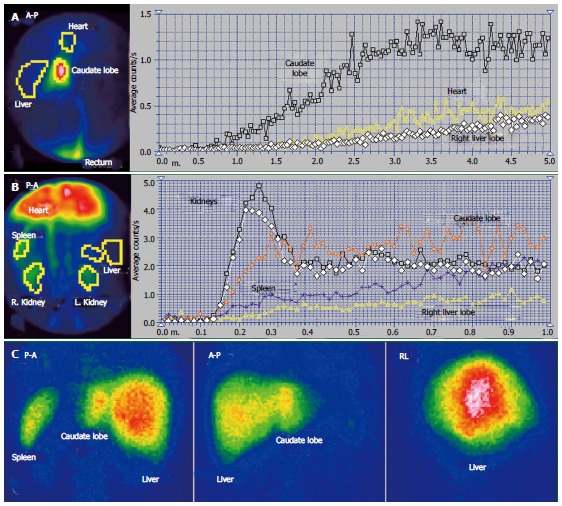
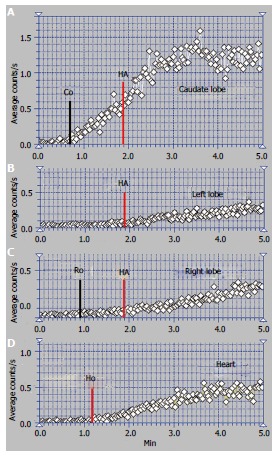
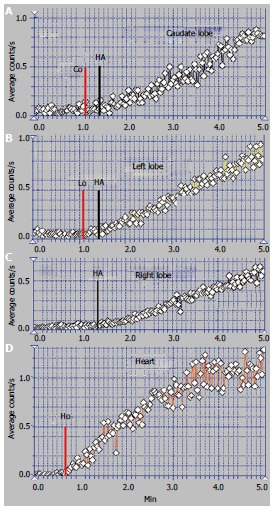
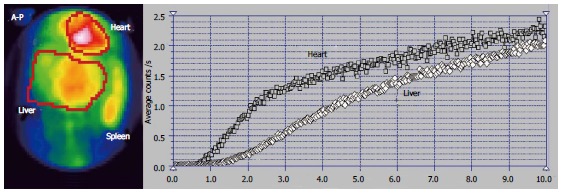
Methods: Fourteen consecutive patients with BCS were evaluated by PRPS between 2003 and 2012. Ten of them underwent LAS and liver scan (LS) with Tc-99m colloid. Eleven patients had clinical manifestations and three were asymptomatic, incidentally diagnosed at PRPS. The control group included 15 healthy subjects. We used new parameters at PRPS, the liver transit time of portal inflow and the blood circulation time between the right heart and liver. PRPS offered information on the hepatic areas missing venous outflow or portal inflow, length and extent of the lesions, open portosystemic shunts (PSS), involvement of the caudate lobe (CL) as an intrahepatic shunt and flow reversal in the splenic vein. LAS was useful in the differential diagnosis between the BCS and portal obstructions, highlighting the hepatic artery buffer response and reversed portal flow. LS offered complementary data, especially on the CL.
Results: We described three hemodynamic categories of the BCS with several subtypes and stages, based on the finding that perfusion changes depend on the initial number and succession in time of the hepatic veins (HVs) obstructions. Obstruction of one hepatic vein (HV) did not cause opening of PSS. The BCS debuted by common obstruction of two HVs had different hemodynamic aspects in acute and chronic stages after subsequent obstruction of the third HV. In chronic stages, obstruction of two HVs resulted in opening of PSS. The BCS, determined by thrombosis of the terminal part of the inferior vena cava, presented in the acute stage with open PSS with low speed flow. At least several weeks are required in the obstructions of two or three HVs for the spontaneous opening of dynamically efficient PSS. The CL seems to have only a transient important role of intrahepatic shunt in several types of the BCS.
Conclusion: Dynamic nuclear medicine investigations assess the extent and length of hepatic venous obstructions, open collaterals, areas without portal inflow, hemodynamic function of the CL and reverse venous flow.
Keywords: Budd-Chiari syndrome; Caudate lobe; Hepatic veins; Liver angioscintigraphy; Per-rectal portal scintigraphy.
Figures

References
-
- Plessier A, Valla DC. Budd-Chiari syndrome. Semin Liver Dis. 2008;28:259–269. - PubMed
-
- Darwish Murad S, Plessier A, Hernandez-Guerra M, Fabris F, Eapen CE, Bahr MJ, Trebicka J, Morard I, Lasser L, Heller J, Hadengue A, Langlet P, Miranda H, Primignani M, Elias E, Leebeek FW, Rosendaal FR, Garcia-Pagan JC, Valla DC, Janssen HL; EN-Vie (European Network for Vascular Disorders of the Liver) Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med. 2009;151:167–175. - PubMed
-
- Janssen HL, Garcia-Pagan JC, Elias E, Mentha G, Hadengue A, Valla DC. Budd-Chiari syndrome: a review by an expert panel. J Hepatol. 2003;38:364–371. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
