

Endovascular and Surgical Treatment of Unruptured MCA Aneurysms: Meta-Analysis and Review of the Literature
- PMID: 24800103
- PMCID: PMC3988829
- DOI: 10.1155/2014/348147
Endovascular and Surgical Treatment of Unruptured MCA Aneurysms: Meta-Analysis and Review of the Literature
Abstract
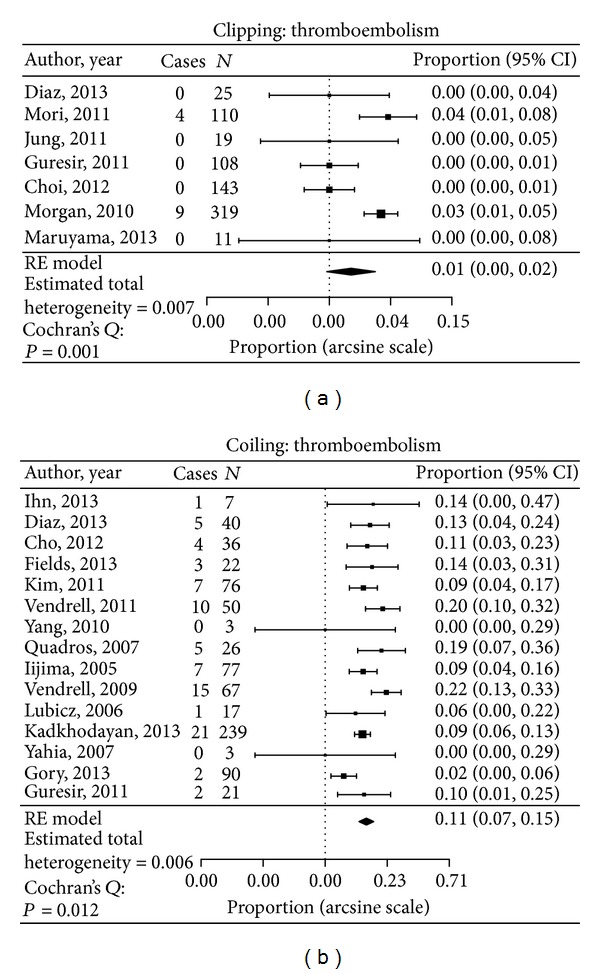
Introduction. The best treatment for unruptured middle cerebral artery (MCA) aneurysms is unclear. We perform a meta-analysis of recent publications to evaluate the results of unruptured MCA aneurysms treated with surgical clipping and endovascular coiling. Methods. A PubMed search for articles published between January 2004 and November 2013 was performed. The R statistical software package was used to create a random effects model for each desired incidence rate. Cochran's Q test was used to evaluate possible heterogeneity among the rates observed in each study. Results. A total of 1891 unruptured MCA aneurysms, 1052 clipped and 839 coiled, were included for analysis. The complete occlusion rate at 6-9 months mean follow-up was 95.5% in the clipped group and 67.8% in the coiled group (P < 0.05). The periprocedural thromboembolism rate in the clipping group was 1.8% compared with 10.7% in the aneurysms treated by coiling (P < 0.05). The recanalization rate was 0% for clipping and 14.3% for coiling (P = 0.05). Modified Rankin scores of 0-2 were obtained in 98.9% of clipped patients compared to 95.5% of coiled (NS). Conclusions. This review weakly supports clipping as the preferred treatment of unruptured MCA aneurysms. Clinical outcomes did not differ significantly between the two groups.
Figures



Similar articles
-
Meta-Analysis of Clipping versus Coiling for the Treatment of Unruptured Middle Cerebral Artery Aneurysms: Direct Comparison of Procedure-Related Complications.Neuropsychiatr Dis Treat. 2019 Dec 5;15:3387-3395. doi: 10.2147/NDT.S226353. eCollection 2019. Neuropsychiatr Dis Treat. 2019. PMID: 31824162 Free PMC article.
-
Endovascular coiling compared with surgical clipping for the treatment of unruptured middle cerebral artery aneurysms: an update.Acta Neurochir Suppl. 2002;82:41-6. doi: 10.1007/978-3-7091-6736-6_8. Acta Neurochir Suppl. 2002. PMID: 12378989
-
Long-term follow-up of unruptured intracranial aneurysms repaired in California.J Neurosurg. 2014 Jun;120(6):1349-57. doi: 10.3171/2014.3.JNS131159. Epub 2014 Apr 11. J Neurosurg. 2014. PMID: 24724850
-
Neuropsychological function after endovascular and neurosurgical treatment of subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2018 Mar;128(3):768-776. doi: 10.3171/2016.11.JNS162055. Epub 2017 Apr 14. J Neurosurg. 2018. PMID: 28409729
-
Endovascular coiling vs. surgical clipping for unruptured intracranial aneurysm: A meta-analysis.Br J Neurosurg. 2015;29(4):485-92. doi: 10.3109/02688697.2015.1023771. Epub 2015 Jun 3. Br J Neurosurg. 2015. PMID: 26037936
Cited by
-
Medicare expenditures for elderly patients undergoing surgical clipping or endovascular intervention for subarachnoid hemorrhage.J Neurosurg. 2017 Mar;126(3):805-810. doi: 10.3171/2016.2.JNS152994. Epub 2016 May 20. J Neurosurg. 2017. PMID: 27203138 Free PMC article.
-
Medicare expenditures for elderly patients undergoing surgical clipping or endovascular intervention for unruptured cerebral aneurysms.J Neurointerv Surg. 2017 Mar;9(3):324-328. doi: 10.1136/neurintsurg-2016-012313. Epub 2016 Mar 24. J Neurointerv Surg. 2017. PMID: 27013232 Free PMC article.
-
Virtual reality guided focused Sylvian approach for clipping unruptured middle cerebral artery aneurysms.Front Surg. 2024 Jul 1;11:1411396. doi: 10.3389/fsurg.2024.1411396. eCollection 2024. Front Surg. 2024. PMID: 39011050 Free PMC article.
-
Clipping versus coiling in unruptured anterior cerebral circulation aneurysms.Surg Neurol Int. 2020 Mar 21;11:50. doi: 10.25259/SNI_1_2020. eCollection 2020. Surg Neurol Int. 2020. PMID: 32257576 Free PMC article.
-
Woven endobridge embolization versus microsurgical clipping for unruptured wide-neck cerebral aneurysms on middle cerebral artery bifurcation.BMC Neurol. 2025 May 8;25(1):202. doi: 10.1186/s12883-025-04199-0. BMC Neurol. 2025. PMID: 40340758 Free PMC article.
References
-
- Molyneux AJ, Kerr RS, Birks J, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): long-term follow-up. The Lancet Neurology. 2009;8(5):427–433. - PMC - PubMed
-
- Qureshi AI, Vazquez G, Tariq N, Suri MFK, Lakshminarayan K, Lanzino G. Impact of International Subarachnoid Aneurysm Trial results on treatment of ruptured intracranial aneurysms in the United States: clinical article. Journal of Neurosurgery. 2011;114(3):834–841. - PubMed
-
- McDonald JS, McDonald RJ, Fan J, Kallmes DF, Lanzino G, Cloft HJ. Comparative effectiveness of unruptured cerebral aneurysm therapies: propensity score analysis of clipping versus coiling. Stroke; A Journal of Cerebral Circulation. 2013;44(4):988–994. - PubMed
-
- Brinjikji W, Rabinstein AA, Lanzino G, Kallmes DF, Cloft HJ. Patient outcomes are better for unruptured cerebral aneurysms treated at centers that preferentially treat with endovascular coiling: a study of the national inpatient sample 2001–2007. American Journal of Neuroradiology. 2011;32(6):1065–1070. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
