

Yellow Fever in Africa: estimating the burden of disease and impact of mass vaccination from outbreak and serological data
- PMID: 24800812
- PMCID: PMC4011853
- DOI: 10.1371/journal.pmed.1001638
Yellow Fever in Africa: estimating the burden of disease and impact of mass vaccination from outbreak and serological data
Abstract
Background: Yellow fever is a vector-borne disease affecting humans and non-human primates in tropical areas of Africa and South America. While eradication is not feasible due to the wildlife reservoir, large scale vaccination activities in Africa during the 1940s to 1960s reduced yellow fever incidence for several decades. However, after a period of low vaccination coverage, yellow fever has resurged in the continent. Since 2006 there has been substantial funding for large preventive mass vaccination campaigns in the most affected countries in Africa to curb the rising burden of disease and control future outbreaks. Contemporary estimates of the yellow fever disease burden are lacking, and the present study aimed to update the previous estimates on the basis of more recent yellow fever occurrence data and improved estimation methods.
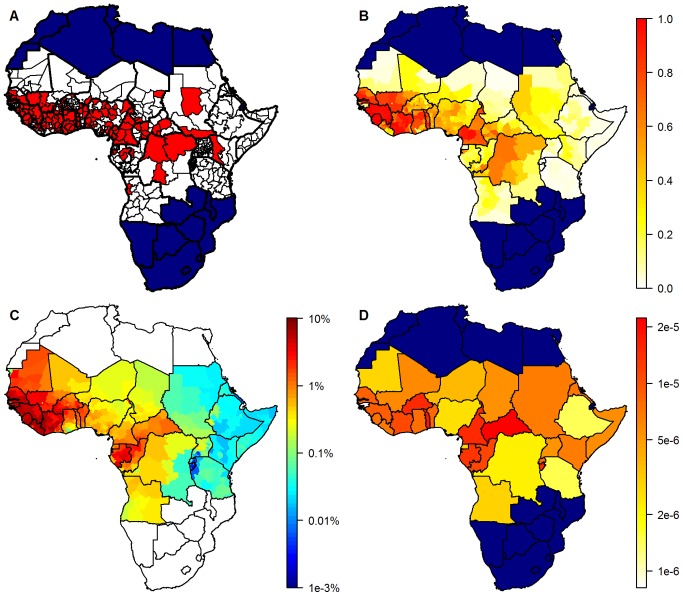
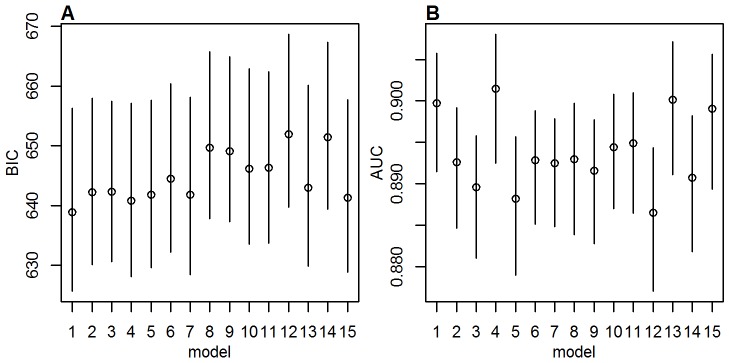
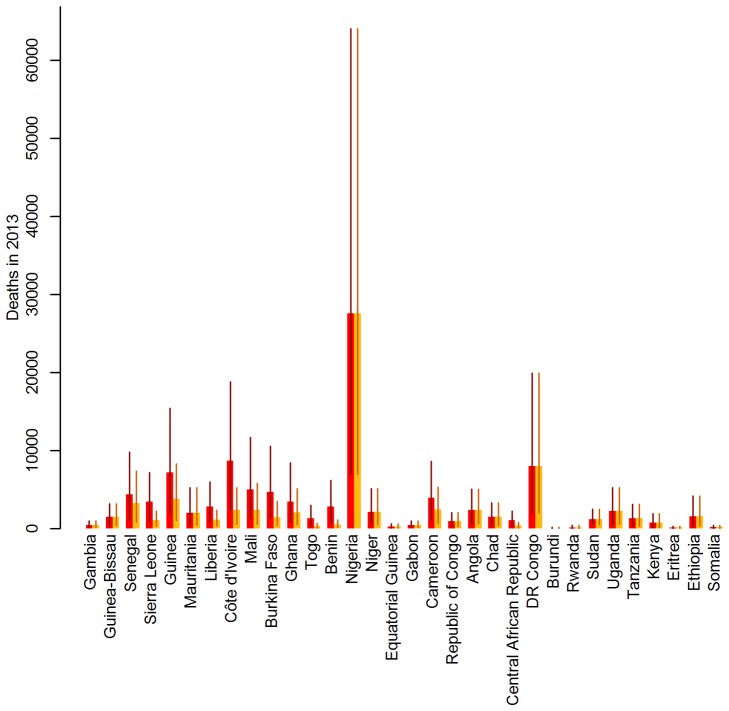
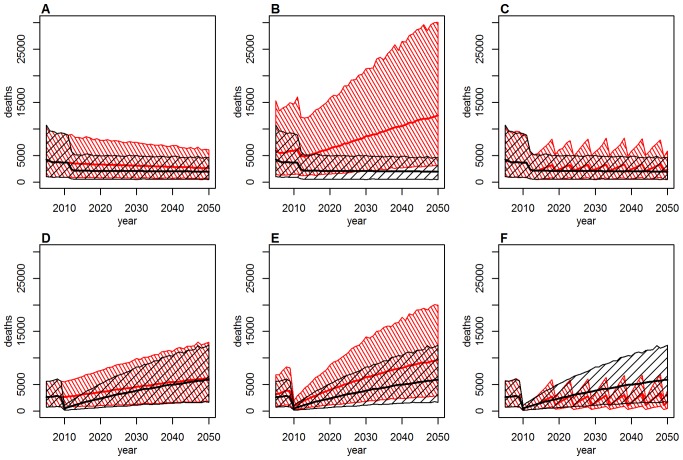
Methods and findings: Generalised linear regression models were fitted to a dataset of the locations of yellow fever outbreaks within the last 25 years to estimate the probability of outbreak reports across the endemic zone. Environmental variables and indicators for the surveillance quality in the affected countries were used as covariates. By comparing probabilities of outbreak reports estimated in the regression with the force of infection estimated for a limited set of locations for which serological surveys were available, the detection probability per case and the force of infection were estimated across the endemic zone. The yellow fever burden in Africa was estimated for the year 2013 as 130,000 (95% CI 51,000-380,000) cases with fever and jaundice or haemorrhage including 78,000 (95% CI 19,000-180,000) deaths, taking into account the current level of vaccination coverage. The impact of the recent mass vaccination campaigns was assessed by evaluating the difference between the estimates obtained for the current vaccination coverage and for a hypothetical scenario excluding these vaccination campaigns. Vaccination campaigns were estimated to have reduced the number of cases and deaths by 27% (95% CI 22%-31%) across the region, achieving up to an 82% reduction in countries targeted by these campaigns. A limitation of our study is the high level of uncertainty in our estimates arising from the sparseness of data available from both surveillance and serological surveys.
Conclusions: With the estimation method presented here, spatial estimates of transmission intensity can be combined with vaccination coverage levels to evaluate the impact of past or proposed vaccination campaigns, thereby helping to allocate resources efficiently for yellow fever control. This method has been used by the Global Alliance for Vaccines and Immunization (GAVI Alliance) to estimate the potential impact of future vaccination campaigns.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Monath TP (2001) Yellow fever: an update. Lancet Infect Dis 1: 11–20. - PubMed
-
- Tomori O (2004) Yellow fever: the recurring plague. Crit Rev Clin Lab Sci 41: 391–427. - PubMed
-
- World Health Organization (1986) Prevention and control of yellow fever in Africa. Geneva: World Health Organization.
-
- World Health Organization (1990) Yellow fever in 1988. Weekly Epidemiological Record 65: 213–219.
-
- World Health Organization. Yellow fever fact sheet no 100. Available: http://www.who.int/mediacentre/factsheets/fs100/en/. Accessed 19 January 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
