

Achieving the HIV prevention impact of voluntary medical male circumcision: lessons and challenges for managing programs
- PMID: 24800840
- PMCID: PMC4011573
- DOI: 10.1371/journal.pmed.1001641
Achieving the HIV prevention impact of voluntary medical male circumcision: lessons and challenges for managing programs
Abstract
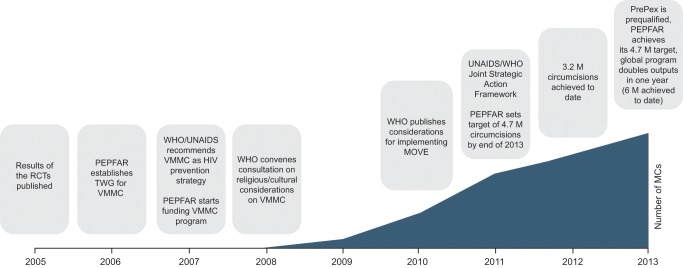
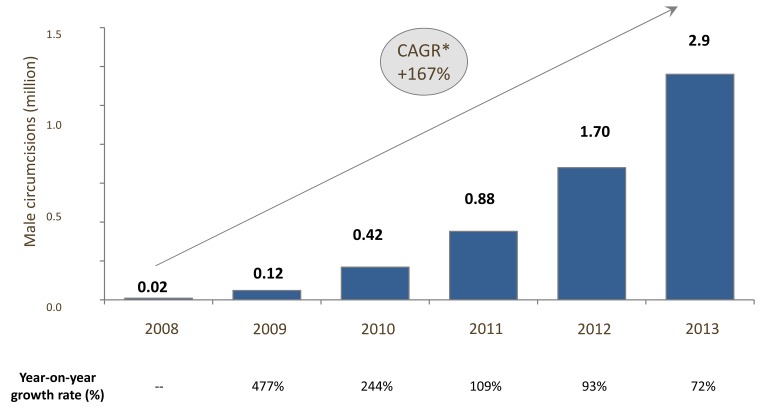
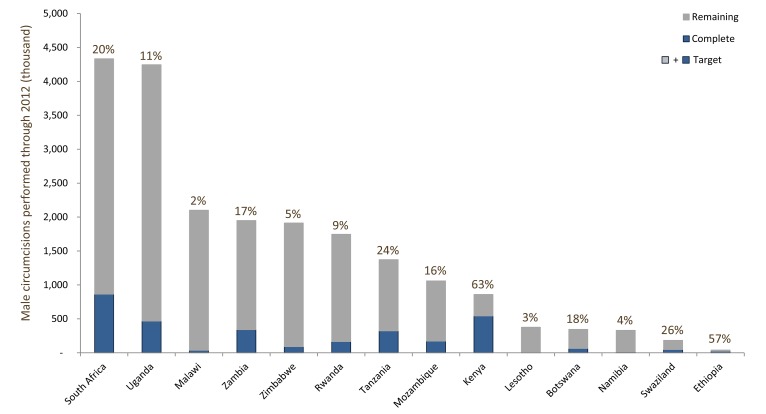
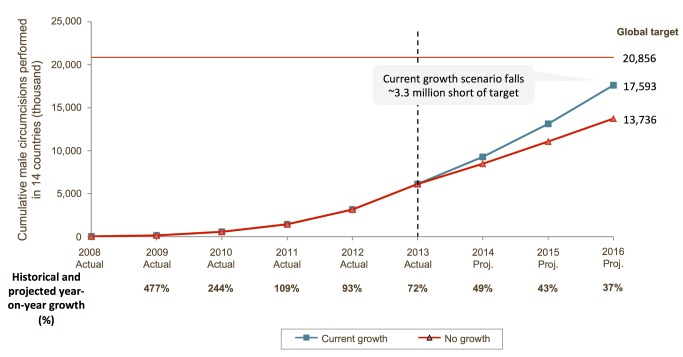
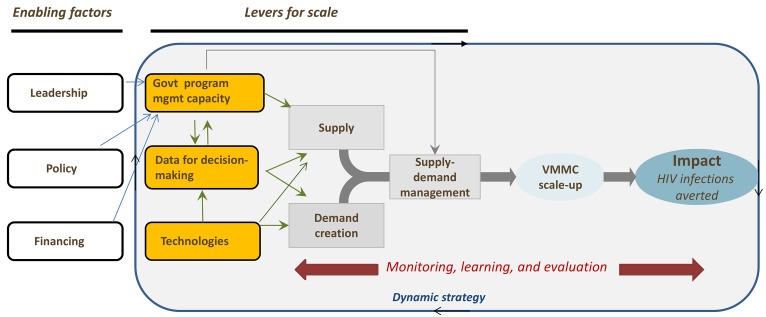
Voluntary medical male circumcision (VMMC) is capable of reducing the risk of sexual transmission of HIV from females to males by approximately 60%. In 2007, the WHO and the Joint United Nations Programme on HIV/AIDS (UNAIDS) recommended making VMMC part of a comprehensive HIV prevention package in countries with a generalized HIV epidemic and low rates of male circumcision. Modeling studies undertaken in 2009-2011 estimated that circumcising 80% of adult males in 14 priority countries in Eastern and Southern Africa within five years, and sustaining coverage levels thereafter, could avert 3.4 million HIV infections within 15 years and save US$16.5 billion in treatment costs. In response, WHO/UNAIDS launched the Joint Strategic Action Framework for accelerating the scale-up of VMMC for HIV prevention in Southern and Eastern Africa, calling for 80% coverage of adult male circumcision by 2016. While VMMC programs have grown dramatically since inception, they appear unlikely to reach this goal. This review provides an overview of findings from the PLOS Collection "Voluntary Medical Male Circumcision for HIV Prevention: Improving Quality, Efficiency, Cost Effectiveness, and Demand for Services during an Accelerated Scale-up." The use of devices for VMMC is also explored. We propose emphasizing management solutions to help VMMC programs in the priority countries achieve the desired impact of averting the greatest possible number of HIV infections. Our recommendations include advocating for prioritization and funding of VMMC, increasing strategic targeting to achieve the goal of reducing HIV incidence, focusing on programmatic efficiency, exploring the role of new technologies, rethinking demand creation, strengthening data use for decision-making, improving governments' program management capacity, strategizing for sustainability, and maintaining a flexible scale-up strategy informed by a strong monitoring, learning, and evaluation platform.
Conflict of interest statement
The authors have declared that no competing interest exist.
Figures
References
-
- Bailey RC, Moses S, Corette BP, Agot K, Maclean I, et al. (2007) Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomized controlled trial. Lancet 369: 643–656. - PubMed
-
- Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, et al. (2007) Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet 369: 657–666. - PubMed
-
- Weiss HA, Quiqley MA, Hayes RJ (2000) Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 14: 2361–2370. - PubMed
-
- WHO, UNAIDS (2007) New data on male circumcision and HIV prevention: Policy and programme implications. WHO/UNAIDS Technical Consultation on Male Circumcision and HIV Prevention: Research Implications for Policy and Programming. Geneva: WHO. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
