

Computed tomographic angiography criteria in the diagnosis of brain death-comparison of sensitivity and interobserver reliability of different evaluation scales
- PMID: 24801451
- PMCID: PMC4125746
- DOI: 10.1007/s00234-014-1364-9
Computed tomographic angiography criteria in the diagnosis of brain death-comparison of sensitivity and interobserver reliability of different evaluation scales
Abstract
Introduction: The standardized diagnostic criteria for computed tomographic angiography (CTA) in diagnosis of brain death (BD) are not yet established. The aim of the study was to compare the sensitivity and interobserver agreement of the three previously used scales of CTA for the diagnosis of BD.
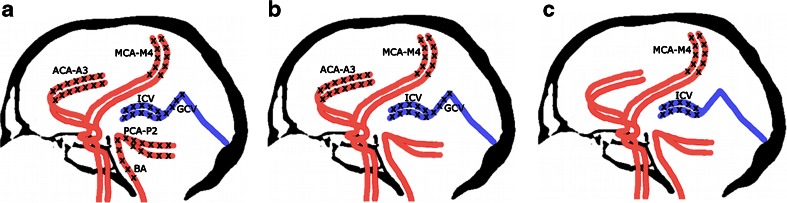
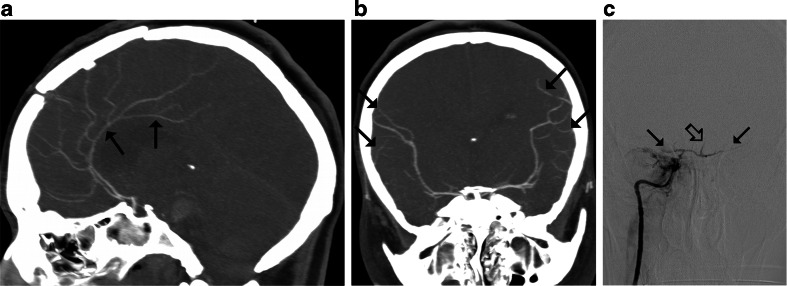
Methods: Eighty-two clinically brain-dead patients underwent CTA with a delay of 40 s after contrast injection. Catheter angiography was used as the reference standard. CTA results were assessed by two radiologists, and the diagnosis of BD was established according to 10-, 7-, and 4-point scales.
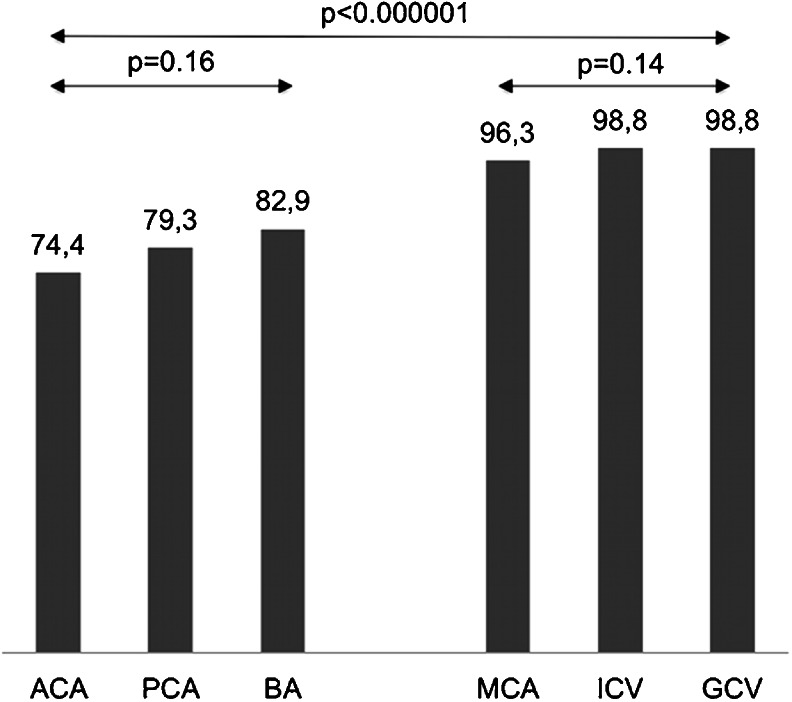
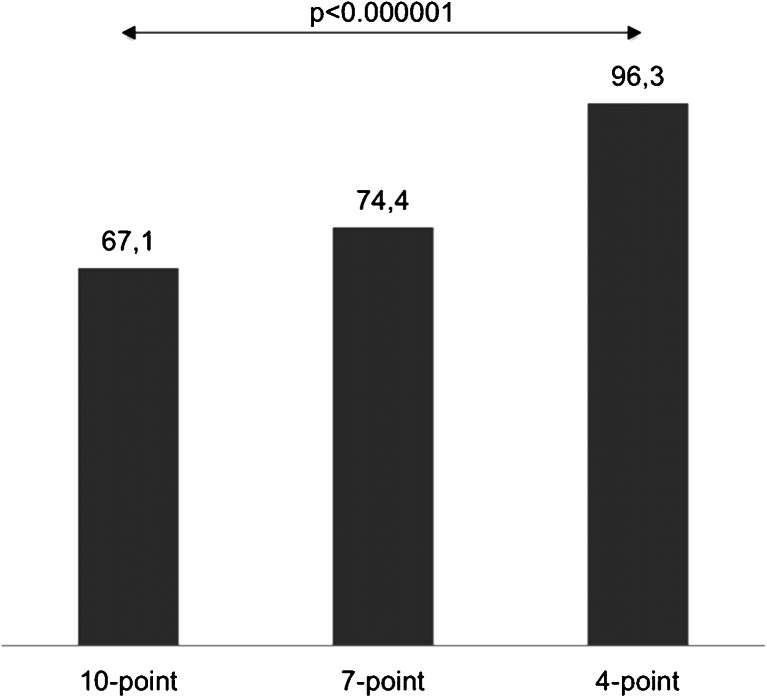
Results: Catheter angiography confirmed the diagnosis of BD in all cases. Opacification of certain cerebral vessels as indicator of BD was highly sensitive: cortical segments of the middle cerebral artery (96.3 %), the internal cerebral vein (98.8 %), and the great cerebral vein (98.8 %). Other vessels were less sensitive: the pericallosal artery (74.4 %), cortical segments of the posterior cerebral artery (79.3 %), and the basilar artery (82.9 %). The sensitivities of the 10-, 7-, and 4-point scales were 67.1, 74.4, and 96.3 %, respectively (p<0.001). Percentage interobserver agreement in diagnosis of BD reached 93 % for the 10-point scale, 89 % for the 7-point scale, and 95 % for the 4-point scale (p=0.37).
Conclusions: In the application of CTA to the diagnosis of BD, reducing the assessment of vascular opacification scale from a 10- to a 4-point scale significantly increases the sensitivity and maintains high interobserver reliability.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
