

Influence of aripiprazole, risperidone, and amisulpride on sensory and sensorimotor gating in healthy 'low and high gating' humans and relation to psychometry
- PMID: 24801767
- PMCID: PMC4138738
- DOI: 10.1038/npp.2014.102
Influence of aripiprazole, risperidone, and amisulpride on sensory and sensorimotor gating in healthy 'low and high gating' humans and relation to psychometry
Abstract
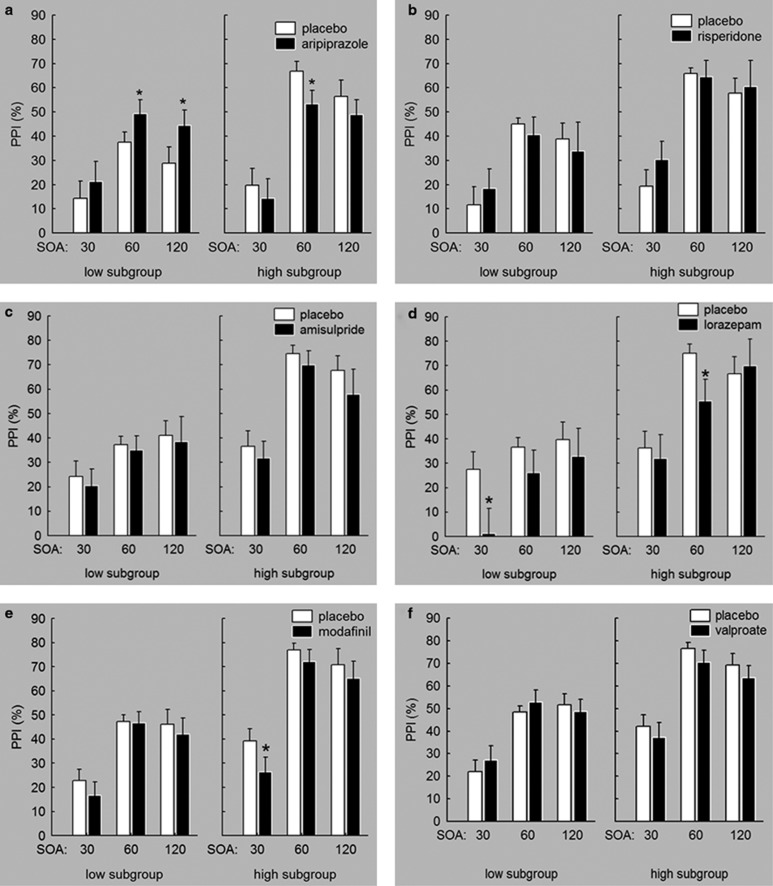
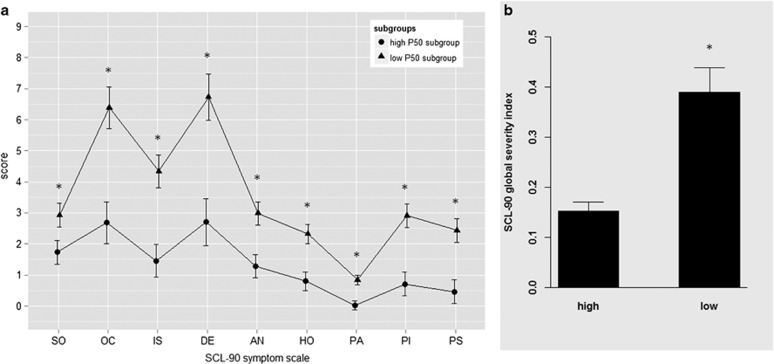
Despite advances in the treatment of schizophrenia spectrum disorders with atypical antipsychotics (AAPs), there is still need for compounds with improved efficacy/side-effect ratios. Evidence from challenge studies suggests that the assessment of gating functions in humans and rodents with naturally low-gating levels might be a useful model to screen for novel compounds with antipsychotic properties. To further evaluate and extend this translational approach, three AAPs were examined. Compounds without antipsychotic properties served as negative control treatments. In a placebo-controlled, within-subject design, healthy males received either single doses of aripiprazole and risperidone (n=28), amisulpride and lorazepam (n=30), or modafinil and valproate (n=30), and placebo. Prepulse inhibiton (PPI) and P50 suppression were assessed. Clinically associated symptoms were evaluated using the SCL-90-R. Aripiprazole, risperidone, and amisulpride increased P50 suppression in low P50 gaters. Lorazepam, modafinil, and valproate did not influence P50 suppression in low gaters. Furthermore, low P50 gaters scored significantly higher on the SCL-90-R than high P50 gaters. Aripiprazole increased PPI in low PPI gaters, whereas modafinil and lorazepam attenuated PPI in both groups. Risperidone, amisulpride, and valproate did not influence PPI. P50 suppression in low gaters appears to be an antipsychotic-sensitive neurophysiologic marker. This conclusion is supported by the association of low P50 suppression and higher clinically associated scores. Furthermore, PPI might be sensitive for atypical mechanisms of antipsychotic medication. The translational model investigating differential effects of AAPs on gating in healthy subjects with naturally low gating can be beneficial for phase II/III development plans by providing additional information for critical decision making.
Figures

Similar articles
-
Effects of dopamine D2/D3 blockade on human sensory and sensorimotor gating in initially antipsychotic-naive, first-episode schizophrenia patients.Neuropsychopharmacology. 2014 Dec;39(13):3000-8. doi: 10.1038/npp.2014.152. Epub 2014 Jul 23. Neuropsychopharmacology. 2014. PMID: 24954063 Free PMC article.
-
Haloperidol differentially modulates prepulse inhibition and p50 suppression in healthy humans stratified for low and high gating levels.Neuropsychopharmacology. 2008 Feb;33(3):497-512. doi: 10.1038/sj.npp.1301421. Epub 2007 Apr 25. Neuropsychopharmacology. 2008. PMID: 17460616 Clinical Trial.
-
Upregulation of adenosine A2A receptors induced by atypical antipsychotics and its correlation with sensory gating in schizophrenia patients.Psychiatry Res. 2012 Dec 30;200(2-3):126-32. doi: 10.1016/j.psychres.2012.04.021. Epub 2012 Jun 16. Psychiatry Res. 2012. PMID: 22705363 Free PMC article.
-
Amisulpride: a review of its use in the management of schizophrenia.Drugs. 2001;61(14):2123-50. doi: 10.2165/00003495-200161140-00014. Drugs. 2001. PMID: 11735643 Review.
-
Spotlight on amisulpride in schizophrenia.CNS Drugs. 2002;16(3):207-11. doi: 10.2165/00023210-200216030-00007. CNS Drugs. 2002. PMID: 11888341 Review.
Cited by
-
The Differential Binding of Antipsychotic Drugs to the ABC Transporter P-Glycoprotein Predicts Cannabinoid-Antipsychotic Drug Interactions.Neuropsychopharmacology. 2017 Oct;42(11):2222-2231. doi: 10.1038/npp.2017.50. Epub 2017 Mar 8. Neuropsychopharmacology. 2017. PMID: 28272498 Free PMC article.
-
Prepulse inhibition in patients with bipolar disorder: a systematic review and meta-analysis.BMC Psychiatry. 2019 Sep 11;19(1):282. doi: 10.1186/s12888-019-2271-8. BMC Psychiatry. 2019. PMID: 31510965 Free PMC article.
-
Investigating the underlying mechanisms of aberrant behaviors in bipolar disorder from patients to models: Rodent and human studies.Neurosci Biobehav Rev. 2015 Nov;58:4-18. doi: 10.1016/j.neubiorev.2015.08.008. Epub 2015 Aug 19. Neurosci Biobehav Rev. 2015. PMID: 26297513 Free PMC article. Review.
-
Spironolactone alleviates schizophrenia-related reversal learning in Tcf4 transgenic mice subjected to social defeat.Schizophrenia (Heidelb). 2022 Sep 29;8(1):77. doi: 10.1038/s41537-022-00290-4. Schizophrenia (Heidelb). 2022. PMID: 36171421 Free PMC article.
-
Therapeutic Potential of Selectively Targeting the α2C-Adrenoceptor in Cognition, Depression, and Schizophrenia-New Developments and Future Perspective.Front Psychiatry. 2017 Aug 14;8:144. doi: 10.3389/fpsyt.2017.00144. eCollection 2017. Front Psychiatry. 2017. PMID: 28855875 Free PMC article. Review.
References
-
- Abduljawad KA, Langley RW, Bradshaw CM, Szabadi E. Effects of bromocriptine and haloperidol on prepulse inhibition: comparison of the acoustic startle eyeblink response and the N1/P2 auditory-evoked response in man. J Psychopharmacol. 1999;13:3–9. - PubMed
-
- Altamura AC, Moliterno D, Paletta S, Maffini M, Mauri MC, Bareggi S. Understanding the pharmacokinetics of anxiolytic drugs. Expert Opin Drug Metab Toxicol. 2013;9:423–440. - PubMed
-
- American Psychiatric Association 1994Diagnostic and Statistical Manual of Mental Disorders: DSM-IV4th ednAmerican Psychiatric Association (APA): Washington, DC
-
- Ballon JS, Feifel D. A systematic review of modafinil: Potential clinical uses and mechanisms of action. J Clin Psychiatry. 2006;67:554–566. - PubMed
-
- Barnes TR, McPhillips MA. Critical analysis and comparison of the side-effect and safety profiles of the new antipsychotics. Br J Psychiatry Suppl. 1999;38:34–43. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
