

Examining continuity of care for Medicaid-enrolled children receiving oral health services in medical offices
- PMID: 24802261
- PMCID: PMC4224632
- DOI: 10.1007/s10995-014-1510-3
Examining continuity of care for Medicaid-enrolled children receiving oral health services in medical offices
Abstract
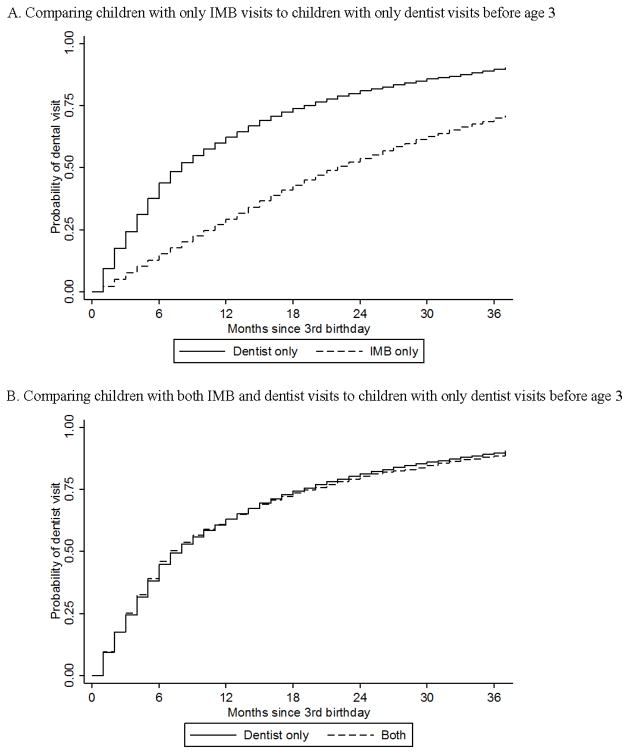
Children living in poverty encounter barriers to dentist visits and disproportionally experience dental caries. To improve access, most state Medicaid programs reimburse pediatric primary care providers for delivering preventive oral health services. To understand continuity of oral health services for children utilizing the North Carolina (NC) Into the Mouths of Babes (IMB) preventive oral health program, we examined the time to a dentist visit after a child's third birthday. This retrospective cohort study used NC Medicaid claims from 2000 to 2006 for 95,578 Medicaid-enrolled children who received oral health services before age 3. We compared children having only dentist visits before age 3 to those with: (1) only IMB visits and (2) both IMB and dentist visits. Cox proportional hazards regression was used to estimate the time to a dentist visit following a child's third birthday. Propensity scores with inverse-probability-of-treatment-weights were used to address confounding. Children with only IMB visits compared to only dentist visits before age 3 had lower rates of dentist visits after their third birthday [adjusted hazard ratio (AHR) = 0.41, 95 % confidence interval (CI) 0.39-0.43]. No difference was observed for children having both IMB and dentist visits and only dentist visits (AHR = 0.99, 95 % CI 0.96-1.03). Barriers to dental care remain as children age, hindering continuity of care for children receiving oral health services in medical offices.
Conflict of interest statement
Figures
Similar articles
-
Preventive Services by Medical and Dental Providers and Treatment Outcomes.J Dent Res. 2014 Jul;93(7):633-8. doi: 10.1177/0022034514536731. Epub 2014 Jun 2. J Dent Res. 2014. PMID: 24891593 Free PMC article.
-
Follow-up preventive dental visits for Medicaid-enrolled children in the medical office.J Public Health Dent. 2008 Summer;68(3):131-8. doi: 10.1111/j.1752-7325.2007.00055.x. J Public Health Dent. 2008. PMID: 18179471 Clinical Trial.
-
Cost-effectiveness of preventive oral health care in medical offices for young Medicaid enrollees.Arch Pediatr Adolesc Med. 2012 Oct;166(10):945-51. doi: 10.1001/archpediatrics.2012.797. Arch Pediatr Adolesc Med. 2012. PMID: 22926203 Free PMC article.
-
Disparities in oral health and access to care: findings of national surveys.Ambul Pediatr. 2002 Mar-Apr;2(2 Suppl):141-7. doi: 10.1367/1539-4409(2002)002<0141:diohaa>2.0.co;2. Ambul Pediatr. 2002. PMID: 11950385 Review.
-
Model to explain dental visit for children aged 0 to 5: Scoping review of birth cohorts.PLoS One. 2025 Jan 8;20(1):e0313922. doi: 10.1371/journal.pone.0313922. eCollection 2025. PLoS One. 2025. PMID: 39774519 Free PMC article.
Cited by
-
Policy interventions to improve the accessibility and affordability of Dutch dental care. A scoping review of effective interventions.Heliyon. 2024 Apr 17;10(9):e28886. doi: 10.1016/j.heliyon.2024.e28886. eCollection 2024 May 15. Heliyon. 2024. PMID: 38707350 Free PMC article.
-
Association between Medicaid expansion, dental coverage policies for adults, and children's receipt of preventive dental services.Health Serv Res. 2020 Oct;55(5):642-650. doi: 10.1111/1475-6773.13324. Epub 2020 Jul 22. Health Serv Res. 2020. PMID: 32700423 Free PMC article.
-
Do Oral Health Services in Medical Offices Replace Pediatric Dental Visits?J Dent Res. 2020 Jul;99(8):891-897. doi: 10.1177/0022034520916161. Epub 2020 Apr 23. J Dent Res. 2020. PMID: 32325007 Free PMC article.
-
Access to preventive services after the integration of oral health care into early childhood education and medical care.J Am Dent Assoc. 2018 Dec;149(12):1024-1031.e2. doi: 10.1016/j.adaj.2018.07.019. Epub 2018 Sep 20. J Am Dent Assoc. 2018. PMID: 30243426 Free PMC article.
-
Impact of Medicaid Policy on the Oral Health of Publicly Insured Children.Matern Child Health J. 2019 Jan;23(1):100-108. doi: 10.1007/s10995-018-2599-6. Matern Child Health J. 2019. PMID: 30032444 Free PMC article.
References
-
- American Academy of Pediatric Dentistry. [Accessed February 8, 2013];Guideline on periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. 2009 http://www.aapd.org/media/Policies_Guidelines/G_Periodicity.pdf. - PubMed
-
- American Academy of Pediatrics. Oral health risk assessment timing and establishment of the dental home. Pediatrics. 2003;111(5):1113–1116. - PubMed
-
- American Dental Association. Baby’s first teeth. J Am Dent Assoc. 2002;133:255. - PubMed
-
- Hakim RB, Babish JD, Davis AC. State of dental care among Medicaid-enrolled children in the united states. Pediatrics. 2012;130(1):5–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
