

Use of coronary artery calcium testing to guide aspirin utilization for primary prevention: estimates from the multi-ethnic study of atherosclerosis
- PMID: 24803472
- PMCID: PMC4412344
- DOI: 10.1161/CIRCOUTCOMES.113.000690
Use of coronary artery calcium testing to guide aspirin utilization for primary prevention: estimates from the multi-ethnic study of atherosclerosis
Abstract
Background: Aspirin for the primary prevention of coronary heart disease (CHD) is only recommended for individuals at high risk for CHD although the majority of CHD events occur in individuals who are at low to intermediate risk.
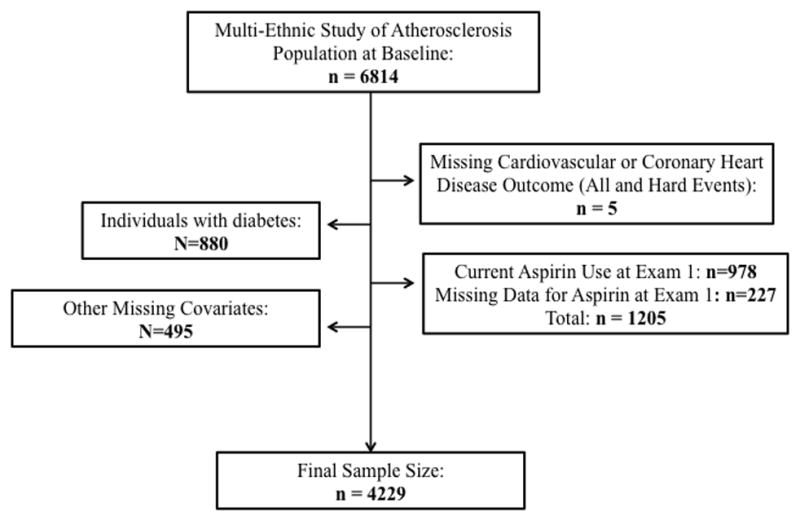
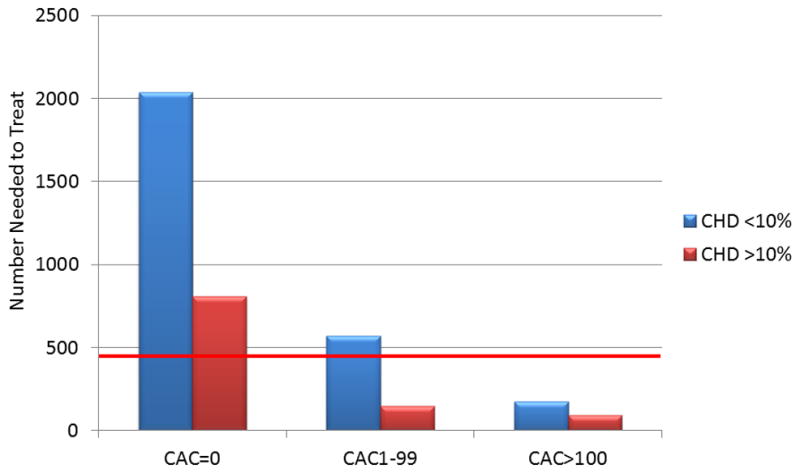
Methods and results: To estimate the potential of coronary artery calcium (CAC) scoring to guide aspirin use for primary prevention of CHD, we studied 4229 participants from the Multi-Ethnic Study of Atherosclerosis who were not on aspirin at baseline and were free of diabetes mellitus. Using data from median 7.6-year follow-up, 5-year number-needed-to-treat estimations were calculated by applying an 18% relative CHD reduction to the observed event rates. This was contrasted to 5-year number-needed-to-harm estimations based on the risk of major bleeding reported in an aspirin meta-analysis. Results were stratified by a 10% 10-year CHD Framingham Risk Score (FRS). Individuals with CAC≥100 had an estimated net benefit with aspirin regardless of their traditional risk status (estimated 5-year number needed to treat of 173 for individuals <10% FRS and 92 for individuals ≥10% FRS, estimated 5-year number needed to harm of 442 for a major bleed). Conversely, individuals with zero CAC had unfavorable estimations (estimated 5-year number needed to treat of 2036 for individuals <10% FRS and 808 for individuals ≥10% FRS, estimated 5-year number needed to harm of 442 for a major bleed). Sex-specific and age-stratified analyses showed similar results.
Conclusions: For the primary prevention of CHD, Multi-Ethnic Study of Atherosclerosis participants with CAC≥100 had favorable risk/benefit estimations for aspirin use while participants with zero CAC were estimated to receive net harm from aspirin.
Keywords: aspirin; coronary disease; prevention.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
Prevention: Aspirin in primary prevention needs individual judgements.Nat Rev Cardiol. 2014 Aug;11(8):438-40. doi: 10.1038/nrcardio.2014.88. Epub 2014 Jun 24. Nat Rev Cardiol. 2014. PMID: 24958081 No abstract available.
References
-
- Cooney MT, Dudina A, Whincup P, Capewell S, Menotti A, Jousilahti P, Njølstad I, Oganov R, Thomsen T, Tverdal A, Wedel H, Wilhelmsen L, Graham I SCORE Investigators. Re-evaluating the Rose approach: comparative benefits of the population and high-risk preventive strategies. Eur J Cardiovasc Prev Rehabil. 2009;16:541–9. - PubMed
-
- Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL. Aspirin for the primary prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized controlled trials. JAMA. 2006;295:306–13. - PubMed
-
- Berger JS, Lala A, Krantz MJ, Baker GS, Hiatt WR. Aspirin for the prevention of cardiovascular events in patients without clinical cardiovascular disease: a meta-analysis of randomized trials. Am Heart J. 2011;162:115–24. - PubMed
-
- Seshasai SR, Wijesuria S, Sivakumaran R, Sivakumaran R, Nethercott S, Ergou S, Sattar N, Ray KK. Effect of aspirin on vascular and nonvascular outcomes: meta-analysis of randomized controlled trials. Arch Int Med. 2012;172:209–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- N01 HC095168/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- N01-HC-95166/HC/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- UL1-RR-025005/RR/NCRR NIH HHS/United States
- N01 HC095167/HC/NHLBI NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- N01-HC-95168/HC/NHLBI NIH HHS/United States
- UL1-RR-024156/RR/NCRR NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- N01 HC095166/HC/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- N01-HC-95167/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
