

Parasite burden and severity of malaria in Tanzanian children
- PMID: 24806160
- PMCID: PMC4091983
- DOI: 10.1056/NEJMoa1303944
Parasite burden and severity of malaria in Tanzanian children
Abstract
Background: Severe Plasmodium falciparum malaria is a major cause of death in children. The contribution of the parasite burden to the pathogenesis of severe malaria has been controversial.
Methods: We documented P. falciparum infection and disease in Tanzanian children followed from birth for an average of 2 years and for as long as 4 years.
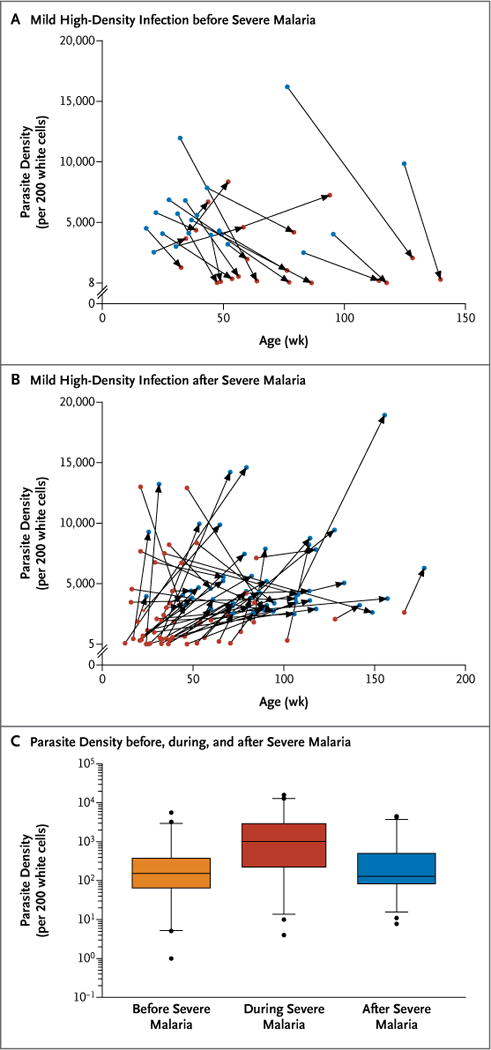
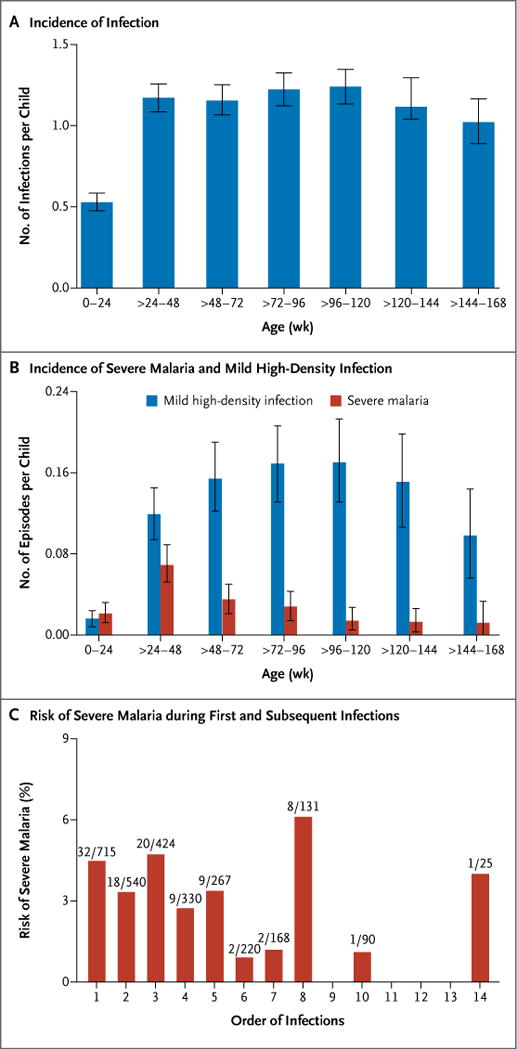
Results: Of the 882 children in our study, 102 had severe malaria, but only 3 had more than two episodes. More than half of first episodes of severe malaria occurred after a second infection. Although parasite levels were higher on average when children had severe rather than mild disease, most children (67 of 102) had high-density infection (>2500 parasites per 200 white cells) with only mild symptoms before severe malaria, after severe malaria, or both. The incidence of severe malaria decreased considerably after infancy, whereas the incidence of high-density infection was similar among all age groups. Infections before and after episodes of severe malaria were associated with similar parasite densities. Nonuse of bed nets, placental malaria at the time of a woman's second or subsequent delivery, high-transmission season, and absence of the sickle cell trait increased severe-malaria risk and parasite density during infections.
Conclusions: Resistance to severe malaria was not acquired after one or two mild infections. Although the parasite burden was higher on average during episodes of severe malaria, a high parasite burden was often insufficient to cause severe malaria even in children who later were susceptible. The diverging rates of severe disease and high-density infection after infancy, as well as the similar parasite burdens before and after severe malaria, indicate that naturally acquired resistance to severe malaria is not explained by improved control of parasite density. (Funded by the National Institute of Allergy and Infectious Diseases and others.).
Figures

Comment in
-
Parasite burden and severity of malaria in Tanzanian children.N Engl J Med. 2014 Jul 31;371(5):482. doi: 10.1056/NEJMc1407114. N Engl J Med. 2014. PMID: 25075849 Free PMC article. No abstract available.
-
Parasite burden and severity of malaria in Tanzanian children.N Engl J Med. 2014 Jul 31;371(5):481-2. doi: 10.1056/NEJMc1407114. N Engl J Med. 2014. PMID: 25075850 No abstract available.
References
-
- World malaria report. Geneva: World Health Organization; 2012.
-
- Greenwood BM, Bradley AK, Greenwood AM, et al. Mortality and morbidity from malaria among children in a rural area of The Gambia, West Africa. Trans R Soc Trop Med Hyg. 1987;81:478–86. - PubMed
-
- Greenwood B, Marsh K, Snow R. Why do some African children develop severe malaria? Parasitol Today. 1991;7:277–81. - PubMed
-
- Mackintosh CL, Beeson JG, Marsh K. Clinical features and pathogenesis of severe malaria. Trends Parasitol. 2004;20:597–603. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources