

Survival on home dialysis in New Zealand
- PMID: 24806458
- PMCID: PMC4013072
- DOI: 10.1371/journal.pone.0096847
Survival on home dialysis in New Zealand
Abstract
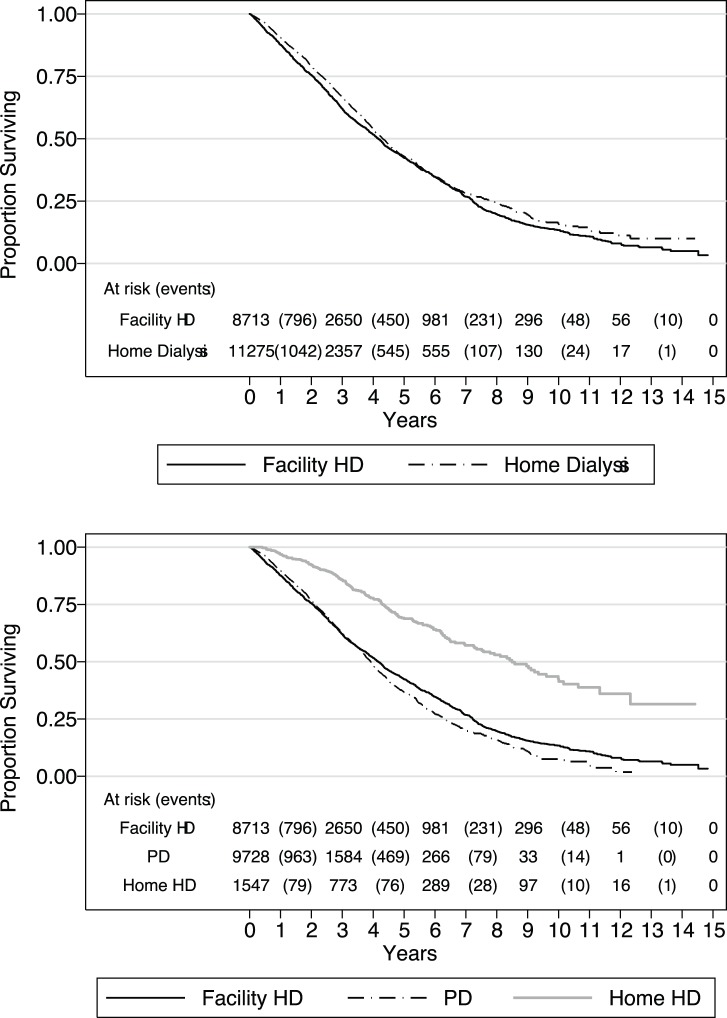
Background: New Zealand (NZ) has a high prevalence of both peritoneal dialysis (PD) and home haemodialysis (HD) relative to other countries, and probably less selection bias. We aimed to determine if home dialysis associates with better survival than facility HD by simultaneous comparisons of the three modalities.
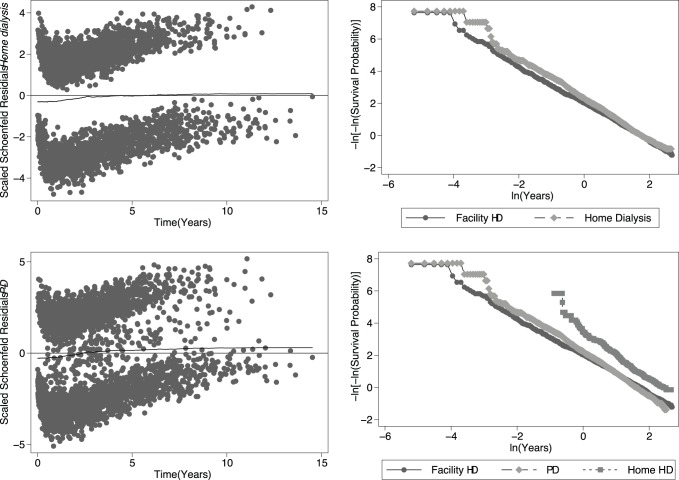
Methods: We analysed survival by time-varying dialysis modality in New Zealanders over a 15-year period to 31-Dec-2011, adjusting for patient co-morbidity by Cox proportional hazards multivariate regression.
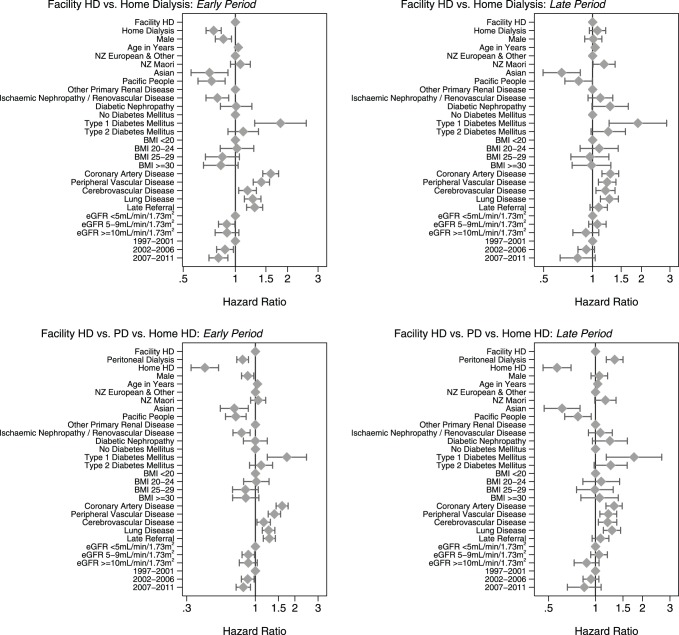
Results: We modelled 6,419 patients with 3,254 deaths over 20,042 patient-years of follow-up. Patients treated with PD and facility HD are similar; those on home HD are younger and healthier. Compared to facility HD, home dialysis (as a unified category) associates with an overall 13% lower mortality risk. Home HD associates with a 52% lower mortality risk. PD associates with a 20% lower mortality risk in the early period (<3 years) that is offset by a 33% greater mortality risk in the late period (>3 years), with no overall net effect. There was effect modification and less observable benefit associated with PD in those with diabetes mellitus, co-morbidity, and in NZ Maori and Pacific People. There was no effect modification by age or by era.
Conclusion: Our study supports the culture of home dialysis in NZ, and suggests that the extent and duration of survival benefit associated with early PD may be greater than appreciated. We are planning further analyses to exclude residual confounding from unmeasured co-morbidity and other sociodemographic factors using database linkage to NZ government datasets. Finally, our results suggest further research into the practice of PD in NZ Maori and Pacific People, as well as definitive study to determine the best timing for switching from PD in the late phase.
Conflict of interest statement
Figures
Similar articles
-
Temporal Changes in Mortality Risk by Dialysis Modality in the Australian and New Zealand Dialysis Population.Am J Kidney Dis. 2015 Sep;66(3):489-98. doi: 10.1053/j.ajkd.2015.03.014. Epub 2015 May 6. Am J Kidney Dis. 2015. PMID: 25958081
-
Home Versus Facility Dialysis and Mortality in Australia and New Zealand.Am J Kidney Dis. 2021 Dec;78(6):826-836.e1. doi: 10.1053/j.ajkd.2021.03.018. Epub 2021 May 13. Am J Kidney Dis. 2021. PMID: 33992726
-
Independent community house hemodialysis as a novel dialysis setting: an observational cohort study.Am J Kidney Dis. 2013 Apr;61(4):598-607. doi: 10.1053/j.ajkd.2012.10.020. Epub 2012 Dec 7. Am J Kidney Dis. 2013. PMID: 23219810
-
The United States' perspectives on home dialysis.Adv Chronic Kidney Dis. 2009 May;16(3):189-97. doi: 10.1053/j.ackd.2009.02.005. Adv Chronic Kidney Dis. 2009. PMID: 19393969 Review.
-
Dialysis Modality and Mortality in the Elderly: A Meta-Analysis.Clin J Am Soc Nephrol. 2015 Jun 5;10(6):983-93. doi: 10.2215/CJN.05160514. Epub 2015 May 4. Clin J Am Soc Nephrol. 2015. PMID: 25941194 Free PMC article. Review.
Cited by
-
Improved long-term survival with home hemodialysis compared with institutional hemodialysis and peritoneal dialysis: a matched cohort study.BMC Nephrol. 2019 Feb 13;20(1):52. doi: 10.1186/s12882-019-1245-x. BMC Nephrol. 2019. PMID: 30760251 Free PMC article.
-
Survival and hospitalization in home versus Institutional hemodialysis-nine years of follow up.J Artif Organs. 2025 May 18. doi: 10.1007/s10047-025-01511-0. Online ahead of print. J Artif Organs. 2025. PMID: 40382760
-
Health economic evaluation of peritoneal dialysis based on cost-effectiveness in Japan: a preliminary study.Clinicoecon Outcomes Res. 2019 Sep 25;11:579-590. doi: 10.2147/CEOR.S212911. eCollection 2019. Clinicoecon Outcomes Res. 2019. PMID: 31576157 Free PMC article.
-
Comparison of peritoneal dialysis with hemodialysis on survival of diabetic patients with end-stage kidney disease: a meta-analysis of cohort studies.Ren Fail. 2019 Nov;41(1):521-531. doi: 10.1080/0886022X.2019.1625788. Ren Fail. 2019. PMID: 31216914 Free PMC article.
-
Similar survival on home haemodialysis and automated peritoneal dialysis: an inception cohort study.Nephrol Dial Transplant. 2022 Jul 26;37(8):1545-1551. doi: 10.1093/ndt/gfab233. Nephrol Dial Transplant. 2022. PMID: 34363472 Free PMC article.
References
-
- Lynn KL, Buttimore AL (2005) Future of home haemodialysis in Australia and New Zealand. Nephrology (Carlton) 10: 231–233. - PubMed
-
- McGregor D, Buttimore A, Robson R, Little P, Morton J, et al. (2000) Thirty years of universal home dialysis in Christchurch. N Z Med J 113: 27–29. - PubMed
-
- Blagg CR (2005) Home haemodialysis: ‘home, home, sweet, sweet home!’. Nephrology (Carlton) 10: 206–214. - PubMed
-
- Marshall MR, Hawley CM, Kerr PG, Polkinghorne KR, Marshall RJ, et al. (2011) Home hemodialysis and mortality risk in Australian and New Zealand populations. Am J Kidney Dis 58: 782–793. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
