

Efficacy and dose-dependent safety of intra-arterial delivery of mesenchymal stem cells in a rodent stroke model
- PMID: 24807059
- PMCID: PMC4012944
- DOI: 10.1371/journal.pone.0093735
Efficacy and dose-dependent safety of intra-arterial delivery of mesenchymal stem cells in a rodent stroke model
Abstract
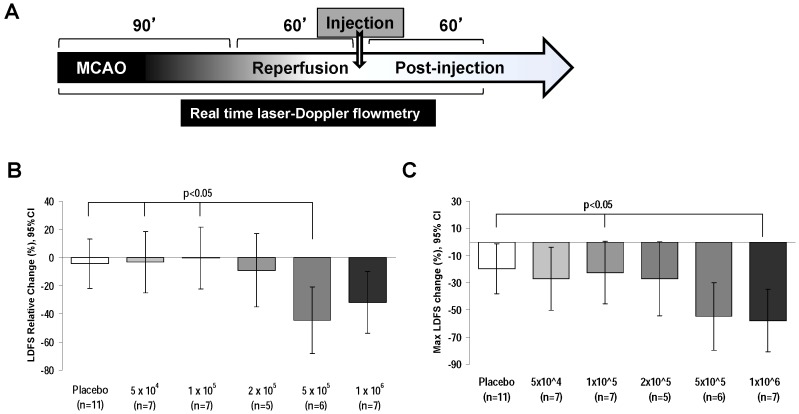
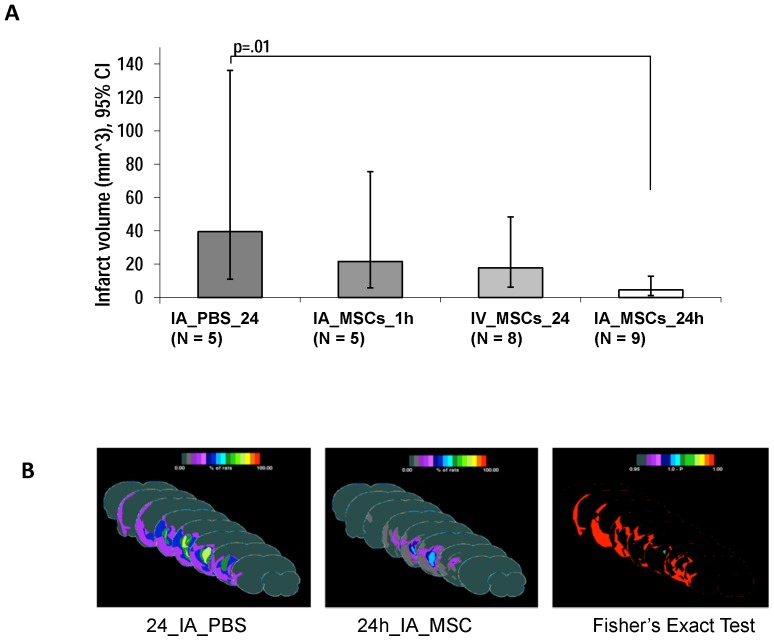
Intra-arterial (IA) delivery of mesenchymal stem cells (MSCs) for acute ischemic stroke is attractive for clinical translation. However, studies using rat model of stroke have demonstrated that IA MSCs delivery can decrease middle cerebral artery (MCA) flow, which may limit its clinical translation. The goal of this study is to identify a dose of IA MSCs (maximum tolerated dose; MTD) that does not compromise MCA flow and evaluate its efficacy and optimal timing in a rat model of reversible middle cerebral artery occlusion (rMCAo). We sought to determine if there is a difference in efficacy of acute (1 h) versus sub-acute (24 h) IA MSCs treatment after rMCAo. Adult female Sprague-Dawley rats underwent rMCAo (90 min) and an hour later a single dose of MSCs (at de-escalating doses 1 × 10(6), 5 × 10(5), 2 × 10(5), 1 × 10(5) and 5 × 10(4)) was given using IA route. MSCs were suspended in phosphate buffered saline (PBS) and PBS alone was used for control experiments. We measured the percent change in mean laser Doppler flow signal over the ipsilateral MCA in de-escalating doses groups to determine MTD. The results demonstrated that the lowering of IA MSC dose to 1 × 10(5) and below did not compromise MCA flow and hence an IA MSC dose of 1 × 10(5) considered as MTD. Subsequently, 1 h and 24 h after rMCAo, rats were treated with IA MSCs or PBS. The 24 h delivery of IA MSCs significantly improved neurodeficit score and reduced the mean infarct volume at one month as compared to control, but not the 1 h delivery. Overall, this study suggests that the IA delivery of MSCs can be performed safely and efficaciously at the MTD of 1 × 10(5) delivered at 24 hours in rodent model of stroke.
Conflict of interest statement
Figures


References
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, et al. (2010) Executive summary: heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation 121: 948–954. - PubMed
-
- Del Zoppo GJ, Saver JL, Jauch EC, Adams HP Jr (2009) American Heart Association Stroke C (2009) Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Stroke 40: 2945–2948. - PMC - PubMed
-
- Del Zoppo GJ, Moskowitz MA (2009) Translating interventions from ischemic stroke models to patients: the view in 2009. Front Neurol Neurosci 25: 34–38. - PubMed
-
- STEPS (2009) Stem Cell Therapies as an Emerging Paradigm in Stroke (STEPS): bridging basic and clinical science for cellular and neurogenic factor therapy in treating stroke. Stroke 40: 510–515. - PubMed
-
- Chen J, Li Y, Wang L, Zhang Z, Lu D, et al. (2001) Therapeutic benefit of intravenous administration of bone marrow stromal cells after cerebral ischemia in rats. Stroke 32: 1005–1011. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
