

Germline BRCA mutation evaluation in a prospective triple-negative breast cancer registry: implications for hereditary breast and/or ovarian cancer syndrome testing
- PMID: 24807107
- PMCID: PMC4171847
- DOI: 10.1007/s10549-014-2980-0
Germline BRCA mutation evaluation in a prospective triple-negative breast cancer registry: implications for hereditary breast and/or ovarian cancer syndrome testing
Abstract
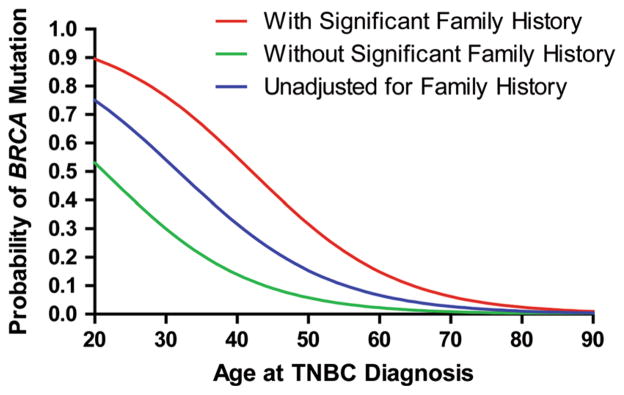
NCCN guidelines recommend genetic testing for all triple-negative breast cancer (TNBC) patients aged ≤60 years. However, due to the lack of prospective information in unselected patients, these guidelines are not uniformly adopted by clinicians and insurance carriers. The aim of this study was to determine the prevalence of BRCA mutations and evaluate the utility of NCCN guidelines in unselected TNBC population. Stage I-IV TNBC patients were enrolled on a prospective registry at academic and community practices. All patients underwent BRCA1/2 testing. Significant family history (SFH) was defined >1 relative with breast cancer at age ≤50 or ≥1 relative with ovarian cancer. Mutation prevalence in the entire cohort and subgroups was calculated. 207 TNBC patients were enrolled between 2011 and 2013. Racial/ethnic distribution: Caucasian (80 %), African-American (14 %), Ashkenazi (1 %). Deleterious BRCA1/2 mutations were identified in 15.4 % (32/207) of patients (BRCA1:11.1 %, BRCA2:4.3 %). SFH reported by 36 % of patients. Mutation prevalence in patients with and without SFH was 31.6 and 6.1 %, respectively. When assessed by age at TNBC diagnosis, the mutation prevalences were 27.6 % (≤50 years), 11.4 % (51-60 years), and 4.9 % (≥61 years). Using SFH or age ≤50 as criteria, 25 and 34 % of mutations, respectively, were missed. Mutation prevalence in patients meeting NCCN guidelines was 18.3 % (32/175) and 0 % (0/32) in patients who did not meet guidelines (p = .0059). In this unselected academic and community population with negligible Ashkenazi representation, we observed an overall BRCA mutation prevalence rate of 15.4 %. BRCA testing based on NCCN guidelines identified all carriers supporting its routine application in clinical practice for TNBC.
Conflict of interest statement
Figures
References
-
- Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O, Borg A, Pasini B, Radice P, Manoukian S, Eccles DM, Tang N, Olah E, Anton-Culver H, Warner E, Lubinski J, Gronwald J, Gorski B, Tulinus H, Thorlacius S, Eerola H, Nevalinna H, Syrjakowski K, Kallioniemi OP, Thompson D, Evans C, Peto J, Lalloo F, Evans DG, Easton DF. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72:1117–1130. doi: 10.1086/375033. - DOI - PMC - PubMed
-
- Mavaddat N, Peock S, Frost D, Ellis S, Platte R, Fineberg E, Evans DG, Izatt L, Eeles RA, Adlard J, Davidson R, Eccles D, Cole T, Cook J, Brewer C, Tischkowits M, Douglas F, Hodgson S, Walker L, Porteous ME, Morrison PJ, Sid LE, Kennedy MJ, Houghton C, Donaldson A, Rogers MT, Dorkins H, Miedzybrodzka Z, Gregory H, Eason J, Barwell J, McCann E, Murray A, Antoniou AC, Easton DF EMBRACE . Cancer risks for BRCA1 and BRCA2 mutation carriers: results from prospective analysis of EMBRACE. J Natl Cancer Inst. 2013;105:812–822. doi: 10.1093/jnci/djt095. - DOI - PubMed
-
- Byrski T, Gronwald J, Huzarski T, Grzbowska E, Budryk M, Stawicka M, Mierzwa T, Szwiec M, Wisniowski R, Siolek M, Dent R, Lubinski J, Narod S. Pathologic complete response rates in young women with BRCA1-positive breast cancers after neoadjuvant chemotherapy. J Clin Oncol. 2010;28:375–379. doi: 10.1200/JCO.2008.20.7019. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
