

Prospective cross-sectional evaluation of the small membrane filtration method for diagnosis of pulmonary tuberculosis
- PMID: 24808236
- PMCID: PMC4097702
- DOI: 10.1128/JCM.00642-14
Prospective cross-sectional evaluation of the small membrane filtration method for diagnosis of pulmonary tuberculosis
Abstract
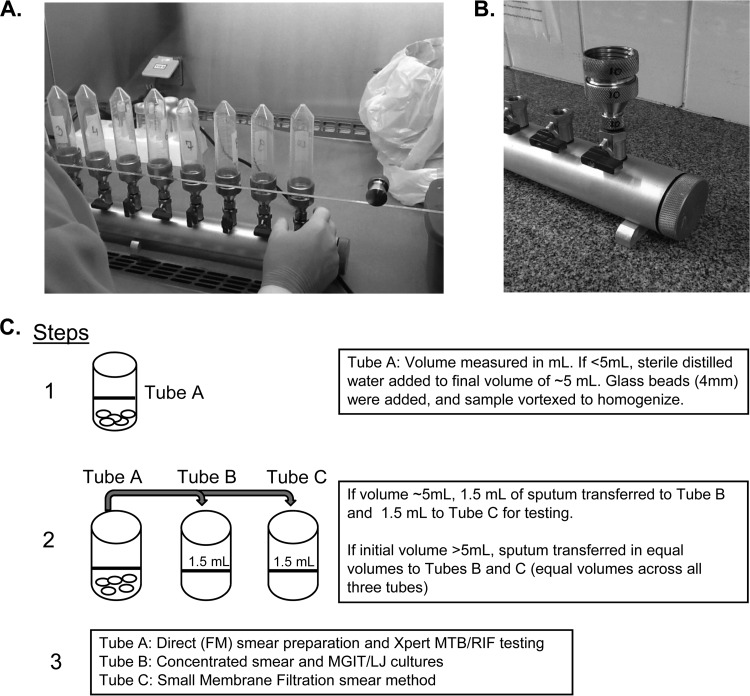
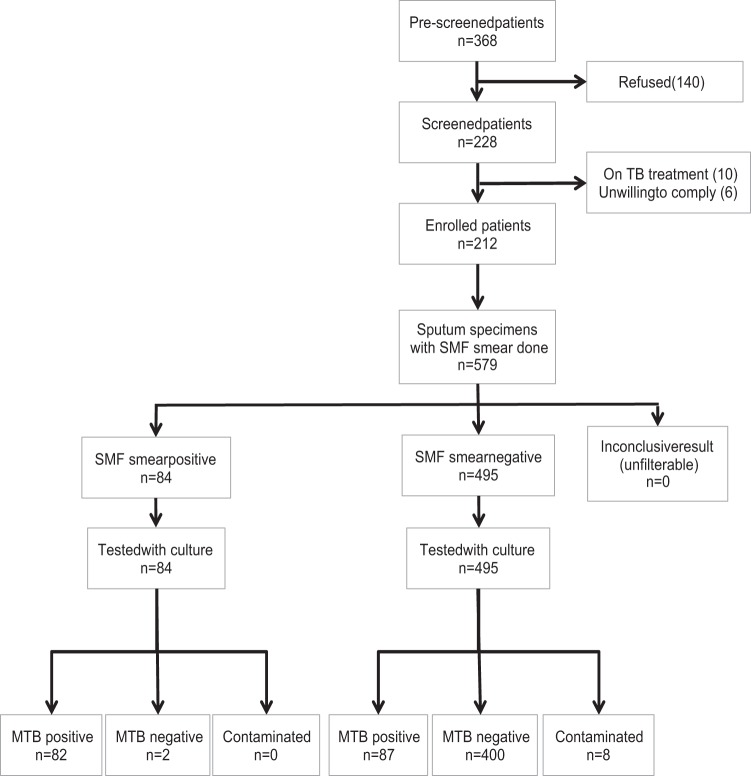
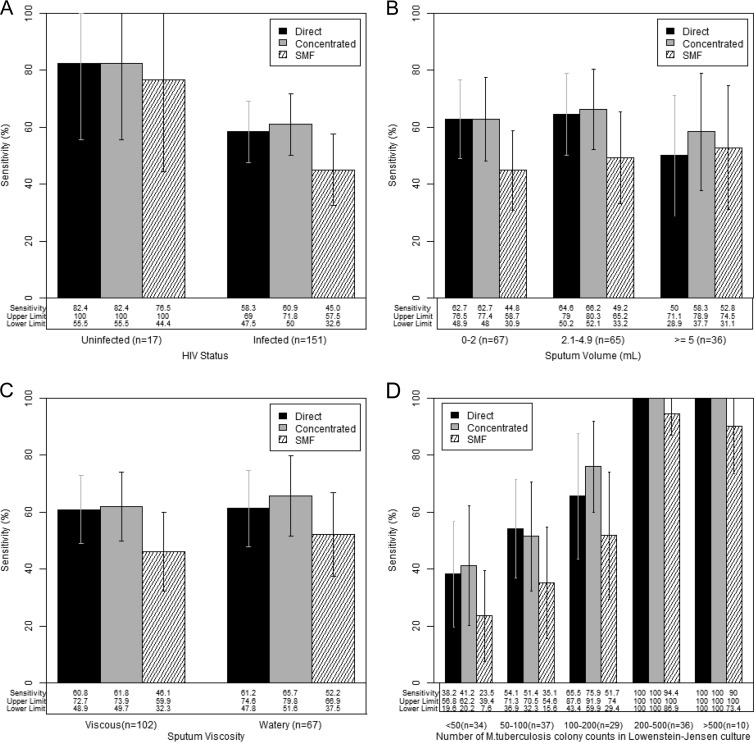
Smear microscopy has suboptimal sensitivity, and there is a need to improve its performance since it is commonly used to diagnose tuberculosis (TB). We prospectively evaluated the diagnostic accuracy of the small membrane filtration (SMF) method, an approach that uses a vacuum manifold and is designed to concentrate bacilli onto a filter that can be examined microscopically. We enrolled hospitalized adults suspected to have pulmonary TB in Kampala, Uganda. We obtained a clinical history and three spontaneously expectorated sputum specimens for smear microscopy (direct, concentrated, and SMF), MGIT (mycobacterial growth indicator tube) 960 and Lowenstein-Jensen (LJ) cultures, and Xpert MTB/RIF testing. We performed per-specimen (primary) and per-patient analyses. From October 2012 to June 2013, we enrolled 212 patients (579 sputum specimens). The participants were mostly female (63.2%), and 81.6% were HIV infected; their median CD4 cell count was 47 cells/μl. Overall, 19.0%, 20.4%, 27.1%, 25.2%, and 25.9% of specimens tested positive by direct smear, concentrated smear, MGIT culture, LJ culture, and Xpert test, respectively. In the per-specimen analysis, the sensitivity of the SMF method (48.5%; 95% confidence interval [CI], 37.4 to 59.6) was lower than those of direct smear (60.9%; 51.4 to 70.5 [P = 0.0001]) and concentrated smear (63.3%; 53.6 to 73.1 [P < 0.0001]). Subgroup analyses showed that SMF performed poorly in specimens having a low volume or low bacterial load. The SMF method performed poorly compared to standard smear techniques and was sensitive to sample preparation techniques. The optimal laboratory SMF protocol may require striking a fine balance between sample dilution and filtration failure rate.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
Comment in
-
Evaluation of a modified small membrane filtration method.J Clin Microbiol. 2014 Dec;52(12):4447. doi: 10.1128/JCM.02567-14. J Clin Microbiol. 2014. PMID: 25398997 Free PMC article. No abstract available.
References
-
- WHO. 2013. Global tuberculosis report 2013. No. WHO/HTM/TB/2013.11. World Health Organization, Geneva, Switzerland: http://www.who.int/tb/publications/global_report/en/
-
- Steingart KR, Ng V, Henry M, Hopewell PC, Ramsay A, Cunningham J, Urbanczik R, Perkins MD, Aziz MA, Pai M. 2006. Sputum processing methods to improve the sensitivity of smear microscopy for tuberculosis: a systematic review. Lancet Infect. Dis. 6:664–674. 10.1016/S1473-3099(06)70602-8 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
