

A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertension
- PMID: 24809339
- PMCID: PMC4251443
- DOI: 10.1136/practneurol-2014-000821
A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertension
Abstract
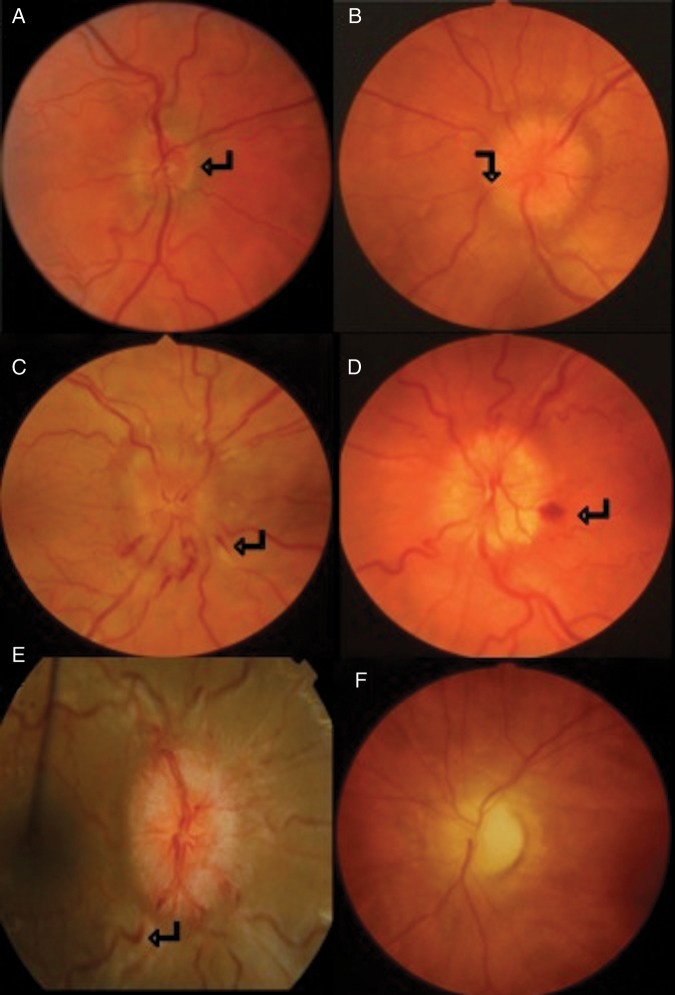
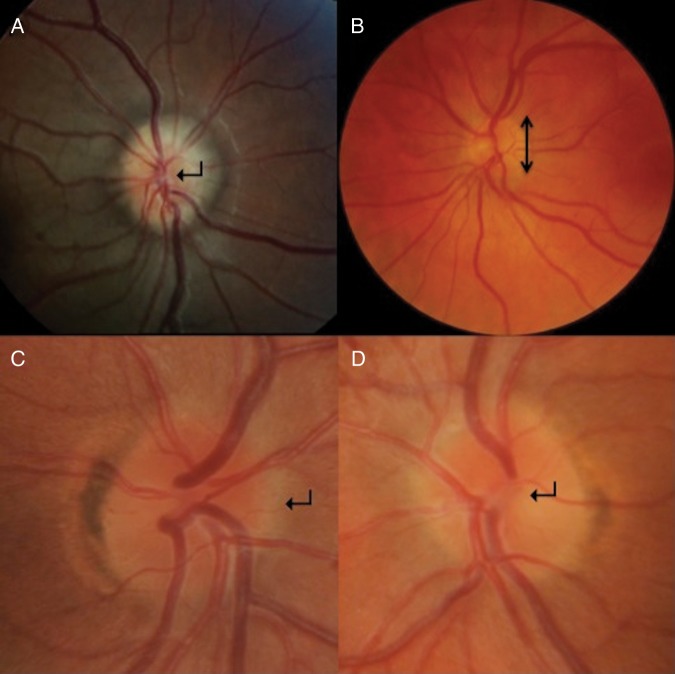
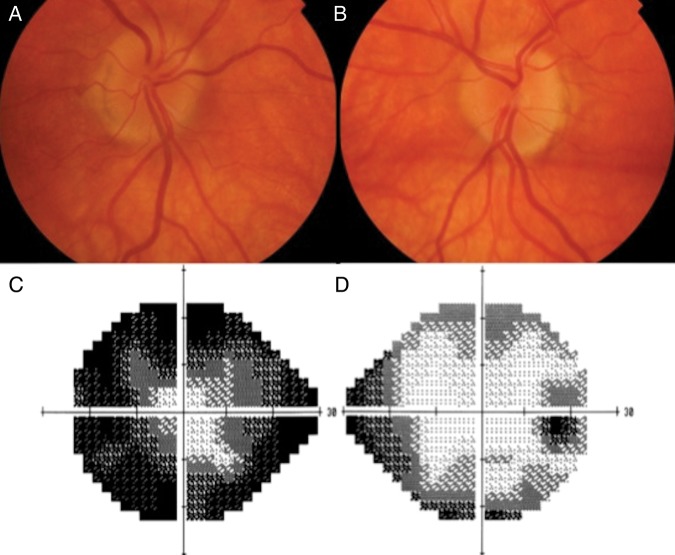
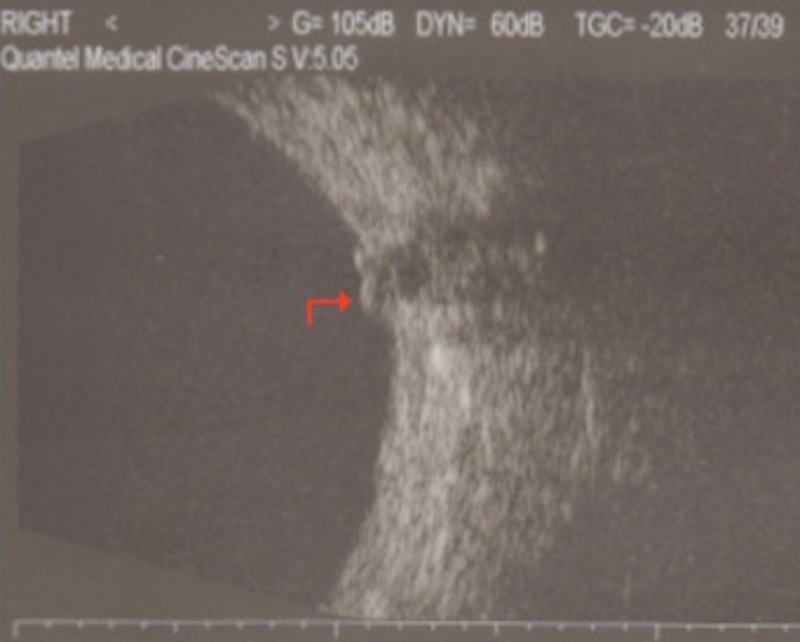
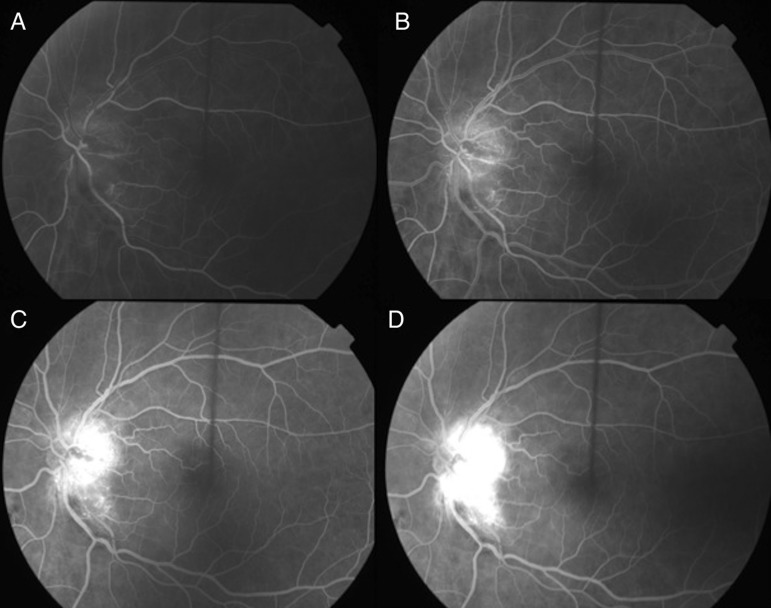
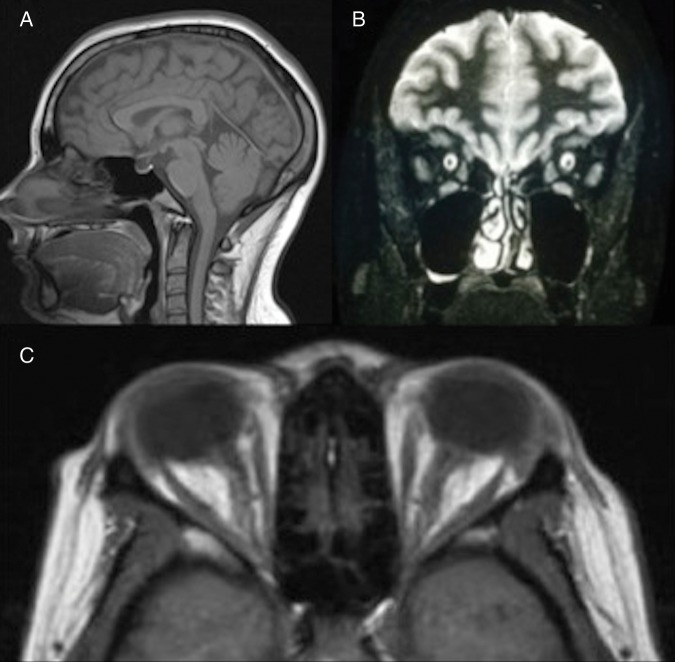
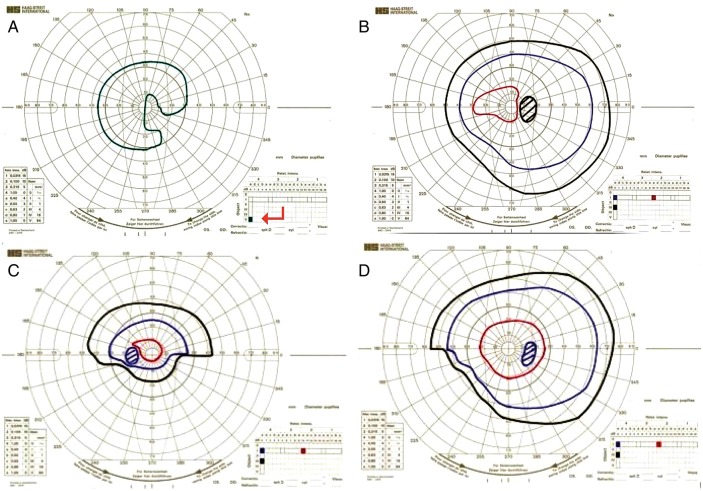
Adult patients who present with papilloedema and symptoms of raised intracranial pressure need urgent multidisciplinary assessment including neuroimaging, to exclude life-threatening causes. Where there is no apparent underlying cause for the raised intracranial pressure, patients are considered to have idiopathic intracranial hypertension (IIH). The incidence of IIH is increasing in line with the global epidemic of obesity. There are controversial issues in its diagnosis and management. This paper gives a practical approach to assessing patients with papilloedema, its investigation and the subsequent management of patients with IIH.
Keywords: HEADACHE; NEUROOPHTHALMOLOGY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures


References
-
- Caballero B. The global epidemic of obesity: an overview. Epidemiol Rev 2007;29:1–5. - PubMed
-
- Corbett JJ, Savino PJ, Thompson HS, et al. Visual loss in pseudotumor cerebri. Follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol 1982;39:461–74. - PubMed
-
- Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2013;81:1159–65. - PubMed
-
- Brodsky MC, Vaphiades M. Magnetic resonance imaging in pseudotumor cerebri. Ophthalmology 1998;105:1686–93. - PubMed
-
- Wright BL, Lai JT, Sinclair AJ. Cerebrospinal fluid and lumbar puncture: a practical review. J Neurol 2012;259:1530–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources