

A care pathway analysis of tuberculosis patients in benin: Highlights on direct costs and critical stages for an evidence-based decision-making
- PMID: 24810007
- PMCID: PMC4014559
- DOI: 10.1371/journal.pone.0096912
A care pathway analysis of tuberculosis patients in benin: Highlights on direct costs and critical stages for an evidence-based decision-making
Abstract
Background: Free tuberculosis control fail to protect patients from substantial medical and non-medical expenditure, thus a greater degree of disaggregation of patient cost is needed to fully capture their context and inform policymaking.
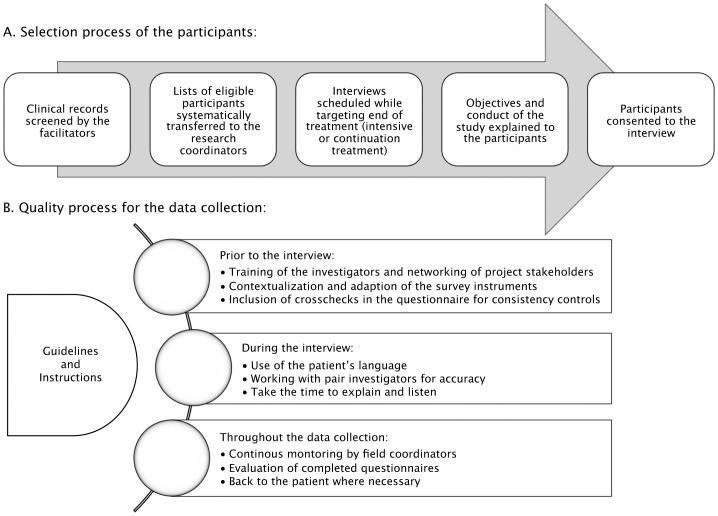
Methods: A retrospective cross-sectional study was conducted on a convenience sample of six health districts of Southern Benin. From August 2008 to February 2009, we recruited all smear-positive pulmonary tuberculosis patients treated under the national strategy in the selected districts. Direct out-of-pocket costs associated with tuberculosis, time delays, and care-seeking pattern were collected from symptom onset to end of treatment.
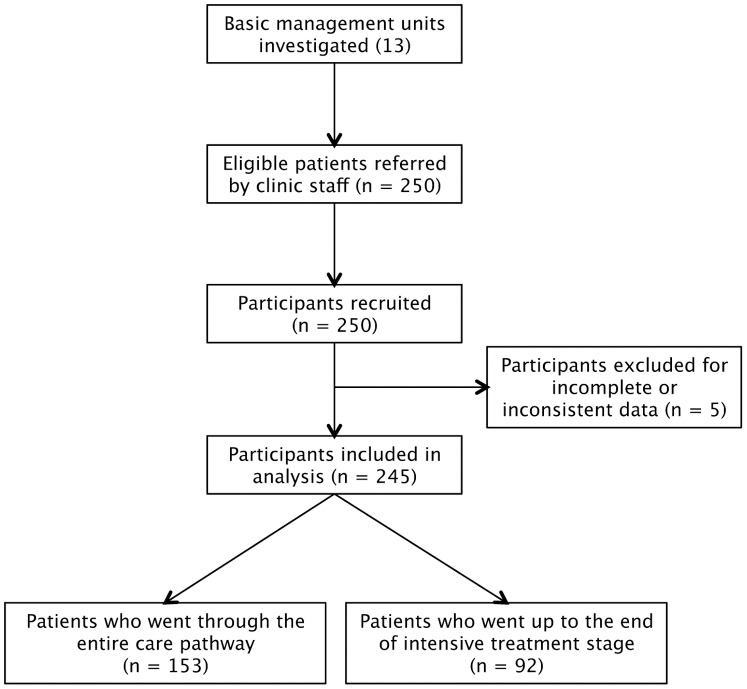
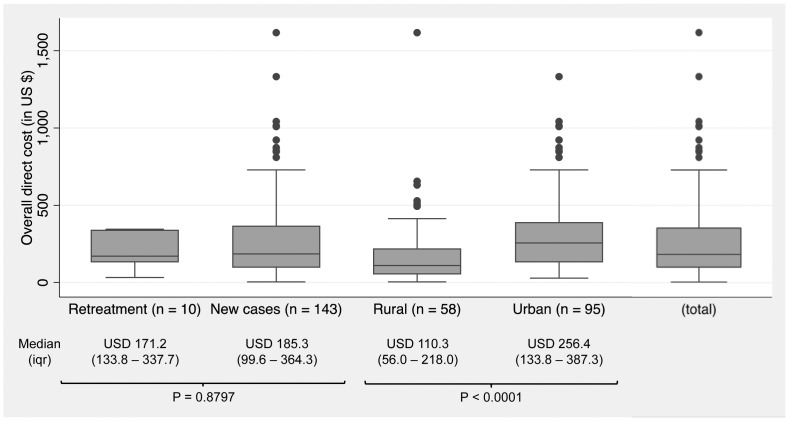
Results: Population description and outcome data were reported for 245 patients of whom 153 completed their care pathway. For them, the median overall direct cost was USD 183 per patient. Payments to traditional healers, self-medication drugs, travel, and food expenditures contributed largely to this cost burden. Patient, provider, and treatment delays were also reported. Pre-diagnosis and intensive treatment stages were the most critical stages, with median expenditure of USD 43 per patient and accounting for 38% and 29% of the overall direct cost, respectively. However, financial barriers differed depending on whether the patient lived in urban or rural areas.
Conclusions: This study delivers new evidence about bottlenecks encountered during the TB care pathway. Financial barriers to accessing the free-of-charge tuberculosis control strategy in Benin remain substantial for low-income households. Irregular time delays and hidden costs, often generated by multiple visits to various care providers, impair appropriate patient pathways. Particular attention should be paid to pre-diagnosis and intensive treatment. Cost assessment and combined targeted interventions embodied by a patient-centered approach on the specific critical stages would likely deliver better program outcomes.
Conflict of interest statement
Figures
References
-
- World Health Organisation (2008) Global tuberculosis control - surveillance, planning, financing. WHO Report. Available: http://www.who.int/tb/publications/global_report/2008/summary/en/index.html. Accessed 2013 March 1.
-
- Gninafon M, Trébucq A, Rieder HL (2011) Epidemiology of tuberculosis in Benin. Int J Tuberc Lung Dis Off J Int Union Tuberc Lung Dis 15: 61–66. - PubMed
-
- WHO (n.d.) The WHO country health profile of Benin. WHO. Available: http://www.who.int/countries/ben/en/. Accessed 2013 Aug 30.
-
- FORESA Study team (2005) Rapport enquête socio-anthropologique sur la prise en charge des patients TB au Bénin. Benin: Institut Régional de Santé Publique (IRSP).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
