

Alternative mechanisms for respiratory syncytial virus (RSV) infection and persistence: could RSV be transmitted through the placenta and persist into developing fetal lungs?
- PMID: 24810284
- PMCID: PMC4065627
- DOI: 10.1016/j.coph.2014.03.008
Alternative mechanisms for respiratory syncytial virus (RSV) infection and persistence: could RSV be transmitted through the placenta and persist into developing fetal lungs?
Abstract
Purpose of review: Respiratory syncytial virus (RSV) represents the most common respiratory pathogen observed worldwide in infants and young children and may play a role in the inception of recurrent wheezing and asthma in childhood. We discuss herein the recent hypothesis that RSV vertically transmitted from the mother to the fetus in utero causes persistent structural and functional changes in the developing lungs of the offspring, thereby predisposing to postnatal airway obstruction.
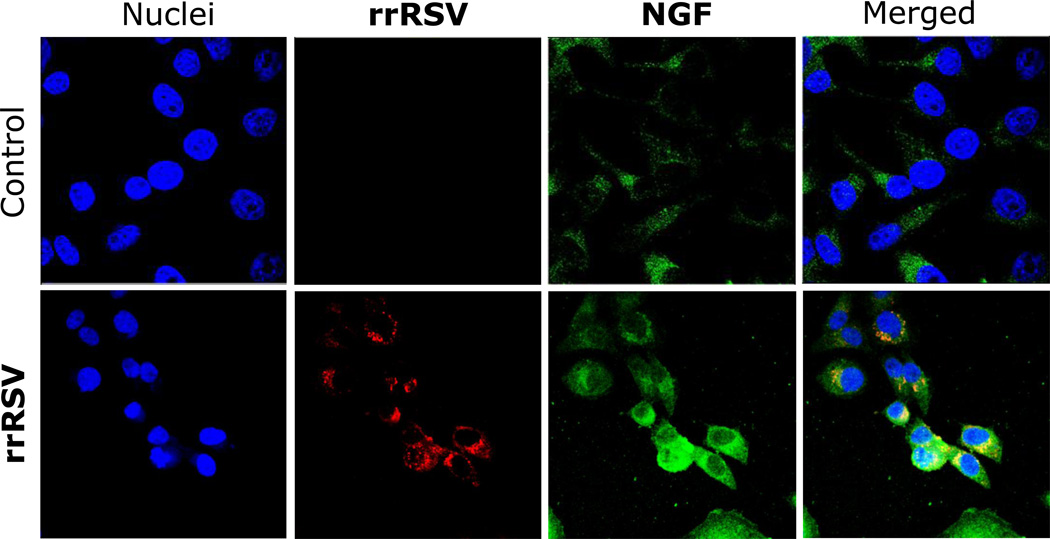
Recent findings: A number of observations in humans support the notion that extrapulmonary tissues may be infected hematogenously by RSV and harbor this virus allowing the persistence of latent infection. More recent data from animal models suggest that RSV can be transmitted across the placenta from the respiratory tract of the mother to that of the fetus, and persist in the lungs both during development, as well as during adulthood. Vertical RSV infection is associated with dysregulation of crucial neurotrophic pathways during ontogenesis, leading to aberrant parasympathetic innervation and airway hyperreactivity after postnatal reinfection.
Summary: These new data challenge the current paradigm that acquisition of RSV infection occurs only after birth and shift attention to the prenatal effects of the virus, with the potential to result in more severe and lasting consequences by interfering with crucial developmental processes. The most immediate implication is that prophylactic strategies targeted to the mother-fetus dyad may reduce the incidence of postviral sequelae like childhood wheezing and asthma.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
There are no conflicts of interest.
Figures



References
-
-
Wright M, Piedimonte G. Respiratory syncytial virus prevention and therapy: past, present, and future. Pediatr Pulmonol. 2011;46:324–347. • A recent comprehensive review of RSV infection.
-
-
- Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B. Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. Am J Respir Crit Care Med. 2000;161:1501–1507. - PubMed
-
- Stein RT, Sherrill D, Morgan WJ, Holberg CJ, Halonen M, Taussig LM, Wright AL, Martinez FD. Respiratory syncytial virus in early life and risk of wheeze and allergy by age 13 years. Lancet. 1999;354:541–545. - PubMed
-
-
Blanken MO, Rovers MM, Molenaar JM, Winkler-Seinstra PL, Meijer A, Kimpen JL, Bont L, Dutch RSV. Neonatal Network: Respiratory syncytial virus and recurrent wheeze in healthy preterm infants. N Engl J Med. 2013;368:1791–1799. •• DBPC trial showing that RSV prophylaxis results in a reduction the incidence of wheezing during the first year of life.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
