

Do-not-resuscitate status and observational comparative effectiveness research in patients with septic shock*
- PMID: 24810532
- PMCID: PMC4266548
- DOI: 10.1097/CCM.0000000000000403
Do-not-resuscitate status and observational comparative effectiveness research in patients with septic shock*
Abstract
Objectives: To assess the importance of including do-not-resuscitate status in critical care observational comparative effectiveness research.
Design: Retrospective analysis.
Setting: All California hospitals participating in the 2007 California State Inpatient Database, which provides do-not-resuscitate status within the first 24 hours of admission.
Patients: Septic shock present at admission.
Interventions: None.
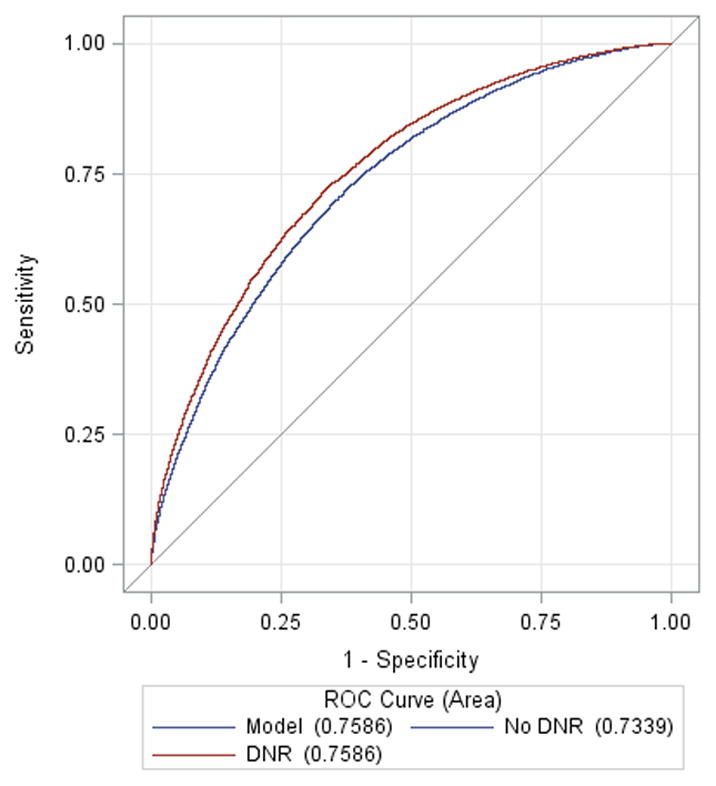
Measurements and main results: We investigated the association of early do-not-resuscitate status with in-hospital mortality among patients with septic shock. We also examined the strength of confounding of do-not-resuscitate status on the association between activated protein C therapy and mortality, an association with conflicting results between observational and randomized studies. We identified 24,408 patients with septic shock; 19.6% had a do-not-resuscitate order. Compared with patients without a do-not-resuscitate order, those with a do-not-resuscitate order were significantly more likely to be older (75 ± 14 vs 67 ± 16 yr) and white (62% vs 53%), with more acute organ failures (1.44 ± 1.15 vs 1.38 ± 1.15), but fewer inpatient interventions (1.0 ± 1.0 vs 1.4 ± 1.1). Adding do-not-resuscitate status to a model with 47 covariates improved mortality discrimination (c-statistic, 0.73-0.76; p < 0.001). Addition of do-not-resuscitate status to a multivariable model assessing the association between activated protein C and mortality resulted in a 9% shift in the activated protein C effect estimate toward the null (odds ratio from 0.78 [95% CI, 0.62-0.99], p = 0.04, to 0.85 [0.67-1.08], p = 0.18).
Conclusions: Among patients with septic shock, do-not-resuscitate status acts as a strong confounder that may inform past discrepancies between observational and randomized studies of activated protein C. Inclusion of early do-not-resuscitate status into more administrative databases may improve observational comparative effectiveness methodology.
Figures

Comment in
-
Why do-not-resuscitate orders matter in comparative effectiveness research*.Crit Care Med. 2014 Sep;42(9):2138-9. doi: 10.1097/CCM.0000000000000450. Crit Care Med. 2014. PMID: 25126803 No abstract available.
References
-
- Lu CY. Observational studies: A review of study designs, challenges and strategies to reduce confounding. Int J Clin Pract. 2009 May;63(5):691–7. - PubMed
-
- Concato J. Study design and “evidence” in patient-oriented research. Am J Respir Crit Care Med. 2013 Jun 1;187(11):1167–72. - PubMed
-
- La Puma J, Silverstein MD, Stocking CB, Roland D, Siegler M. Life-sustaining treatment. A prospective study of patients with DNR orders in a teaching hospital. Arch Intern Med. 1988 Oct;148(10):2193–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
