

Predisposing risk factors for delirium in living donor liver transplantation patients in intensive care units
- PMID: 24811254
- PMCID: PMC4014540
- DOI: 10.1371/journal.pone.0096676
Predisposing risk factors for delirium in living donor liver transplantation patients in intensive care units
Abstract
Background: Delirium is one of the main causes of increased length of intensive care unit (ICU) stay among patients who have undergone living donor liver transplantation (LDLT). We aimed to evaluate risk factors for delirium after LDLT as well as to investigate whether delirium impacts the length of ICU and hospital stay.
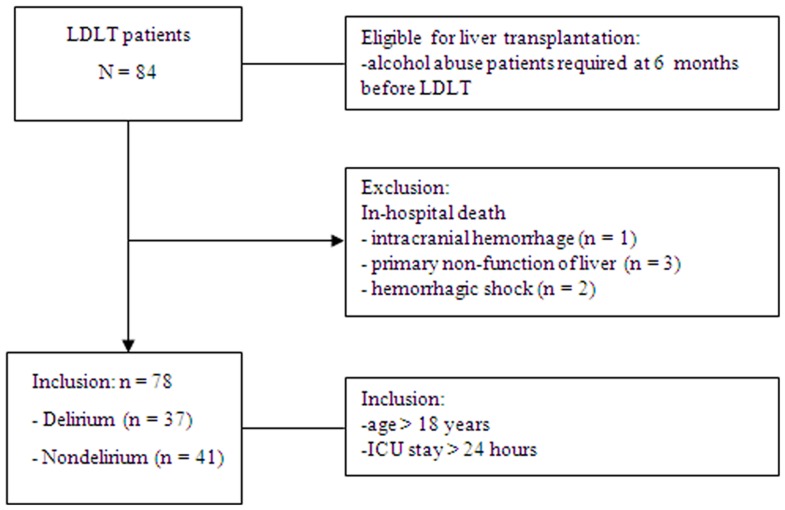
Methods: Seventy-eight patients who underwent LDLT during the period January 2010 to December 2012 at a single medical center were enrolled. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) scale was used to diagnose delirium. Preoperative, postoperative, and hematologic factors were included as potential risk factors for developing delirium.
Results: During the study period, delirium was diagnosed in 37 (47.4%) patients after LDLT. The mean onset of symptoms occurred 7.0±5.5 days after surgery and the mean duration of symptoms was 5.0±2.6 days. The length of stay in the ICU for patients with delirium (39.8±28.1 days) was significantly longer than that for patients without delirium (29.3±19.0 days) (p<0.05). Risk factors associated with delirium included history of alcohol abuse [odds ratio (OR) = 6.40, 95% confidence interval (CI): 1.85-22.06], preoperative hepatic encephalopathy (OR = 4.45, 95% CI: 1.36-14.51), APACHE II score ≥16 (OR = 1.73, 95% CI: 1.71-2.56), and duration of endotracheal intubation ≥5 days (OR = 1.81, 95% CI: 1.52-2.23).
Conclusions: History of alcohol abuse, preoperative hepatic encephalopathy, APACHE II scores ≥16 and endotracheal intubation ≥5 days were predictive of developing delirium in the ICU following liver transplantation surgery and were associated with increased length of ICU and hospital stay.
Conflict of interest statement
References
-
- Ely EW, Inouye SK, Bernard GR, Gordon S, Francis J, et al. (2001) Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit(CAM-ICU). JAMA 286: 2703–2710. - PubMed
-
- Pisani MA, Murphy TE, Van Ness PH, Araujo KLB, Inouye SK (2007) Characteristics associated with delirium in older patients in a medical intensive care unit. Arch Intern Med 167: 1629–1634. - PubMed
-
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, et al. (2004) Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 291: 1753–1762. - PubMed
-
- Shehabi Y, Riker RR, Bokesch PM, Wisemandle W, Shintani A, et al. (2010) Delirium duration and mortality in lightly sedated, mechanically ventilated intensive care patients. Crit Care Med 38: 2311–2318. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
