

Zanamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments
- PMID: 24811412
- PMCID: PMC3981976
- DOI: 10.1136/bmj.g2547
Zanamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments
Abstract
Objectives: To describe the potential benefits and harms of zanamivir.
Design: Systematic review of clinical study reports of randomised placebo controlled trials and regulatory information
Data sources: Clinical study reports, trial registries, electronic databases, regulatory archives, and correspondence with manufacturers.
Eligibility criteria for selecting studies: Randomised placebo controlled trials in adults and children who had confirmed or suspected exposure to natural influenza.
Main outcome measures: Time to first alleviation of symptoms, influenza outcomes and complications, admissions to hospital, and adverse events in the intention to treat (ITT) population.
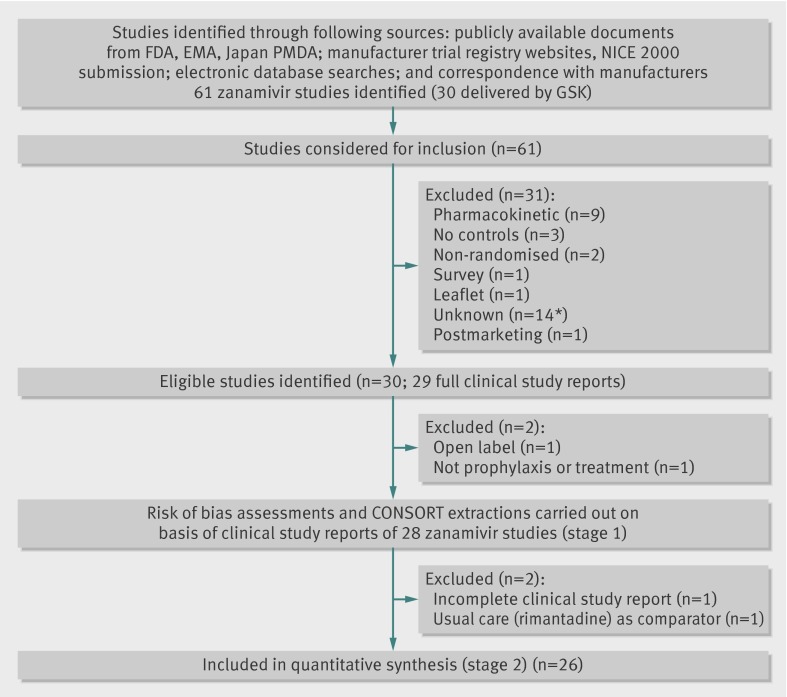
Results: We included 28 trials in stage 1 (judgment of appropriate study design) and 26 in stage 2 (formal analysis). For treatment of adults, zanamivir reduced the time to first alleviation of symptoms of influenza-like illness by 0.60 days (95% confidence interval 0.39 to 0.81, P<0.001, I(2)=9%), which equates to an average 14.4 hours' reduction, or a 10% reduction in mean duration of symptoms from 6.6 days to 6.0 days. Time to first alleviation of symptoms was shorter in all participants when any relief drugs were allowed compared with no use. Zanamivir did not reduce the risk of self reported investigator mediated pneumonia (risk difference 0.17%, -0.73% to 0.70%) or radiologically confirmed pneumonia (-0.06%, -6.56% to 2.11%) in adults. The effect on pneumonia in children was also not significant (0.56%, -1.64% to 1.04%). There was no significant effect on otitis media or sinusitis in both adults and children, with only a small effect noted for bronchitis in adults (1.80%, 0.65% to 2.80%), but not in children. There were no data to assess effects on admissions in adults and children. Zanamivir tended to be well tolerated. In zanamivir prophylaxis studies, symptomatic influenza in individuals was significantly reduced (1.98%, (0.98% to 2.54%); reducing event rates from 3.26% to 1.27%, which means 51 people need to be treated to prevent one influenza case (95% confidence interval, 40 to 103). In contrast, the prophylaxis effect on asymptomatic influenza cases was not significant in individuals (risk difference 0.14%, -1.10% to 1.10%) or in households (1.32%, -2.20% to 3.84%). In households treated prophylactically there was an effect on symptomatic influenza (14.84%, 12.18% to 16.55%), but this was based on only two small studies including 824 participants. Prophylaxis in adults reduced unverified pneumonia (0.32%, 0.09% to 0.41%; NNTB (number needed to treat to benefit) 311, 244 to 1086) but had no effect on pneumonia in children or on bronchitis or sinusitis in adults or children (risk difference 0.32%, 0.09% to 0.41%; NNTB 311, 244 to 1086).
Conclusions: Based on a full assessment of all trials conducted, zanamivir reduces the time to symptomatic improvement in adults (but not in children) with influenza-like illness by just over half a day, although this effect might be attenuated by symptom relief medication. Zanamivir also reduces the proportion of patients with laboratory confirmed symptomatic influenza. We found no evidence that zanamivir reduces the risk of complications of influenza, particularly pneumonia, or the risk of hospital admission or death. Its harmful effects were minor (except for bronchospasm), perhaps because of low bioavailability.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Cochrane review questions effectiveness of neuraminidase inhibitors.BMJ. 2014 Apr 9;348:g2675. doi: 10.1136/bmj.g2675. BMJ. 2014. PMID: 24721619 No abstract available.
-
Zanamivir for influenza in adults and children shows limited benefit for treatment of symptomatic influenza and no effect on relevant complications.Evid Based Med. 2015 Feb;20(1):7. doi: 10.1136/ebmed-2014-110046. Epub 2014 Sep 16. Evid Based Med. 2015. PMID: 25228674 No abstract available.
References
-
- Jefferson T, Jones MA, Doshi P, Del Mar CB, Heneghan CJ, Hama R, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev 2012;1:CD008965. - PubMed
-
- Requesting Relenza data. www.bmj.com/open-data/relenza.
-
- TA168 Influenza—zanamivir, amantadine and oseltamivir (review): guidance. 2 2 www.nice.org.uk/nicemedia/live/11774/43268/43268.pdf
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical