

Subclinical miliary Mycobacterium bovis following BCG immunotherapy for transitional cell carcinoma of the bladder
- PMID: 24811557
- PMCID: PMC4024537
- DOI: 10.1136/bcr-2013-201202
Subclinical miliary Mycobacterium bovis following BCG immunotherapy for transitional cell carcinoma of the bladder
Abstract
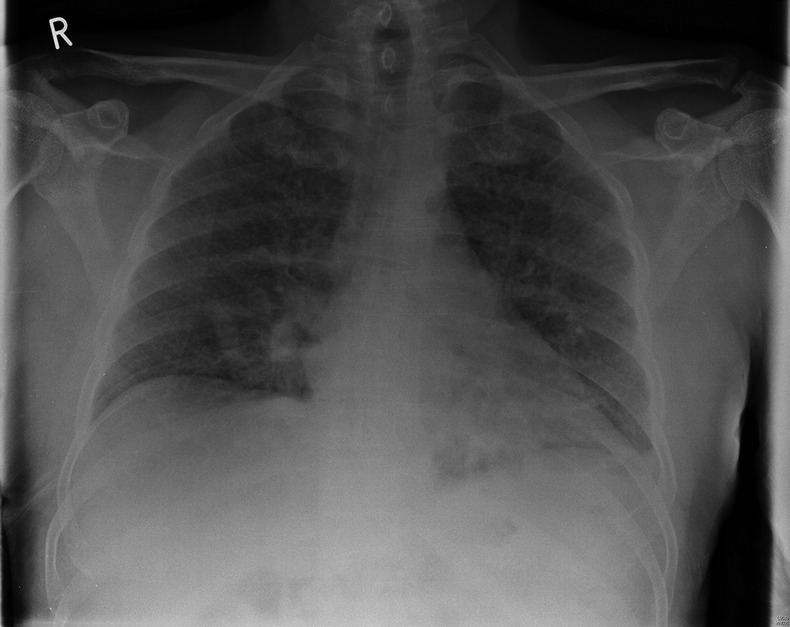
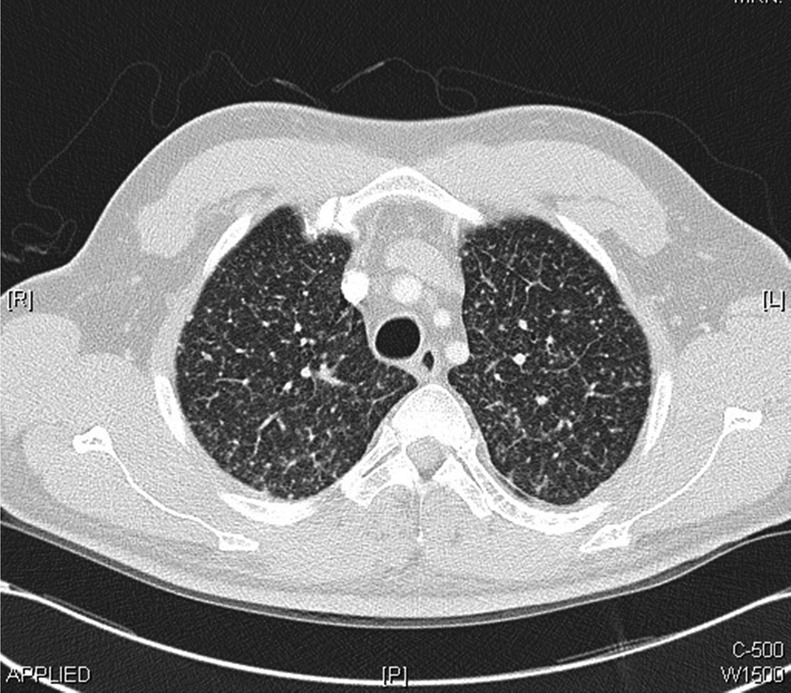
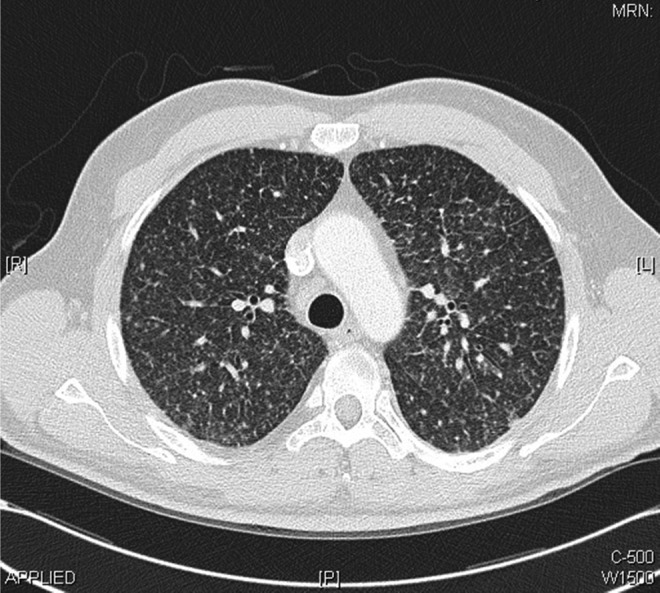
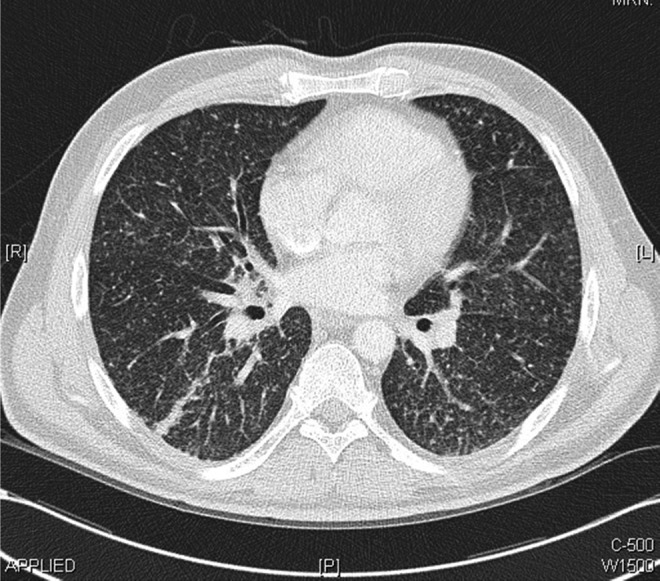
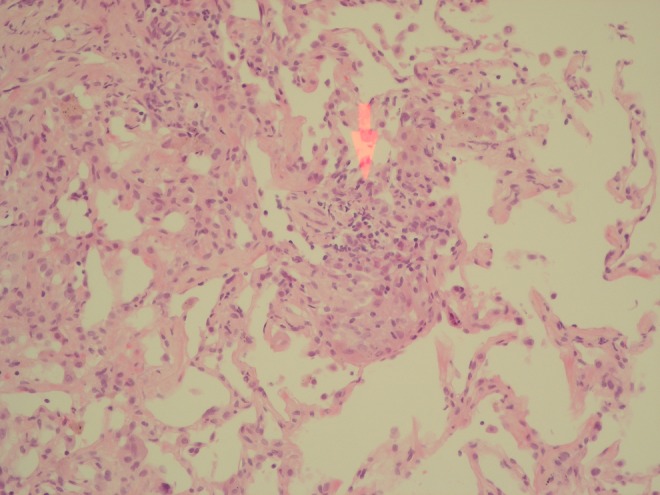
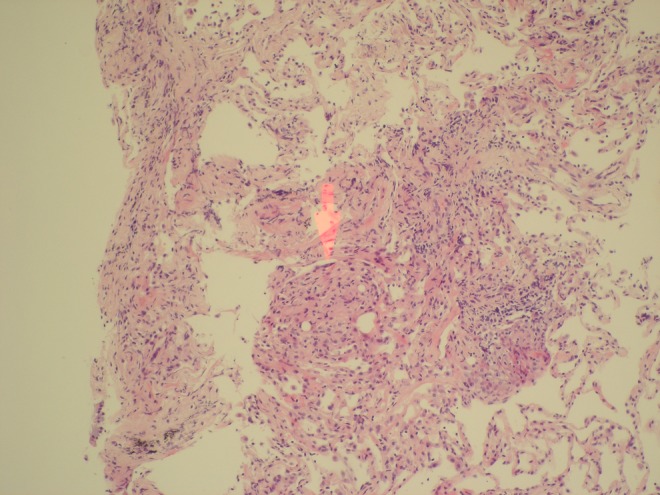
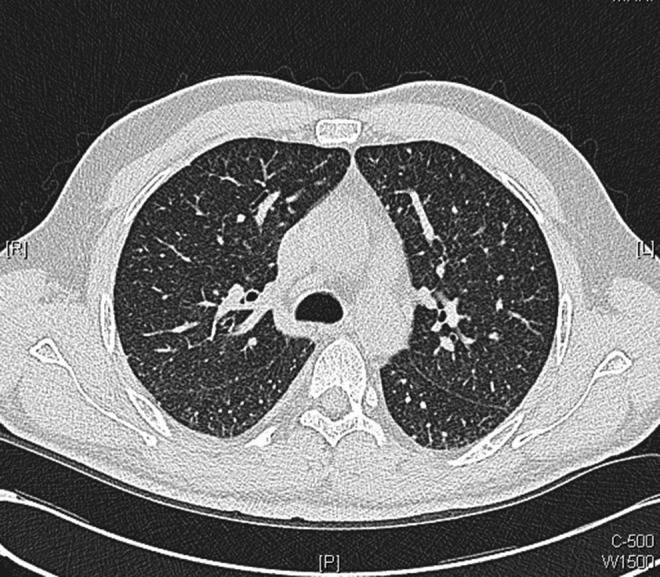
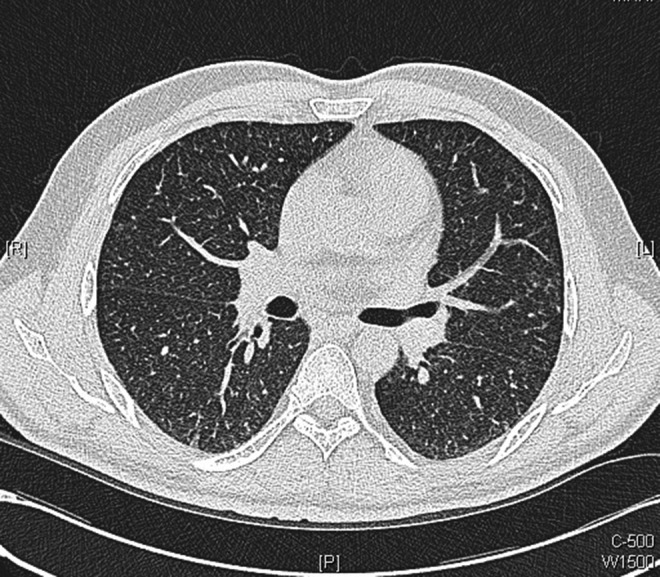
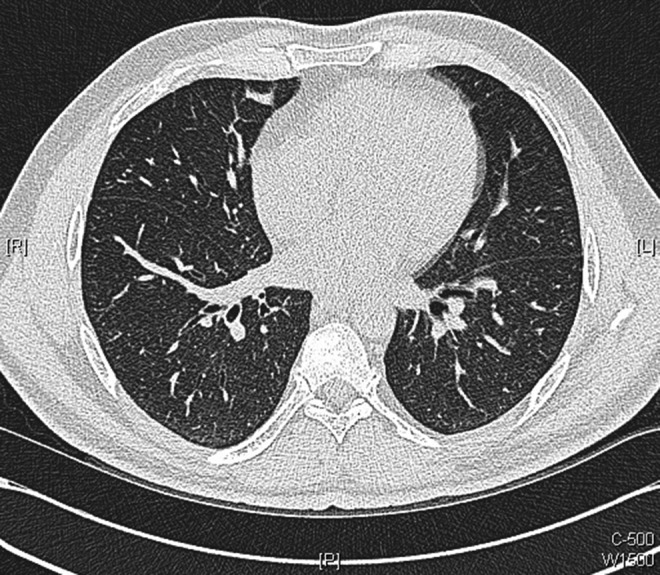
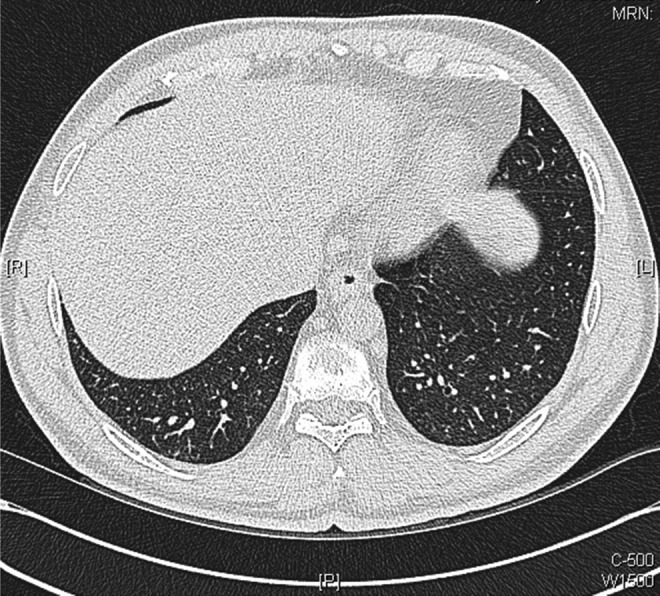
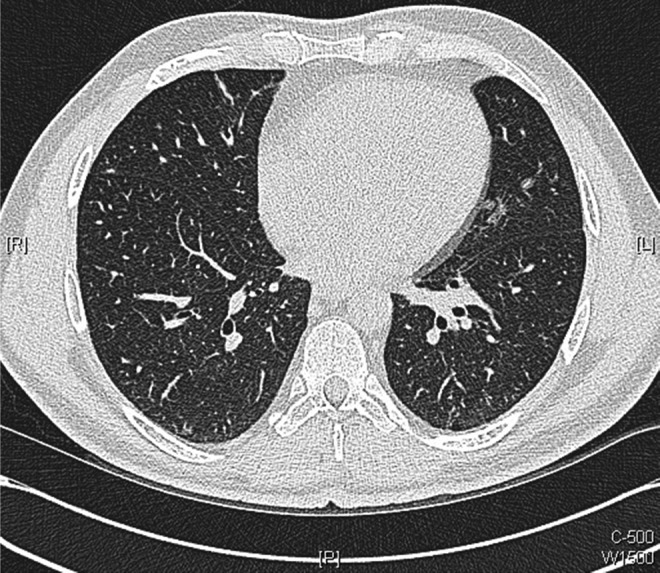
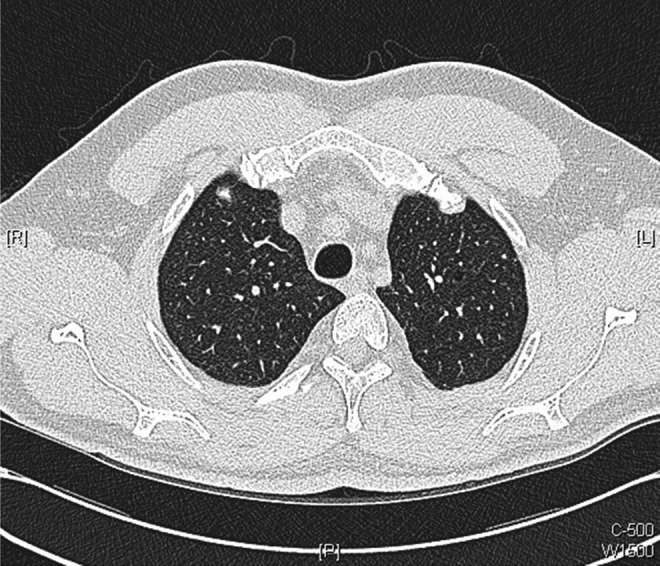
The authors present an unusual case of a 51-year-old man who developed relatively mild non-specific symptoms following intravesical BCG instillation for superficial transitional cell carcinoma of the bladder, with radiological investigations demonstrating typical features of miliary tuberculosis (TB). Transbronchial biopsy showed small foci of poorly formed granuloma suggestive of Mycobacterium infection. The patient's respiratory symptoms only became apparent 7 days after discharge having had 4 weeks of unremarkable inpatient stay where he remained clinically well. Prompt anti-TB treatment resulted in a remarkable improvement in his symptoms and radiological appearance, supporting the diagnosis of disseminated Mycobacterium bovis infection. This case highlights the importance of recognising miliary M bovis as a potential complication in patients receiving BCG immunotherapy, and that the disease course can be subclinical with delayed onset of symptoms.
Figures

Similar articles
-
Miliary Mycobacterium bovis induced by intravesical bacille Calmette-Guérin immunotherapy.Am Rev Respir Dis. 1992 Nov;146(5 Pt 1):1330-3. doi: 10.1164/ajrccm/146.5_Pt_1.1330. Am Rev Respir Dis. 1992. PMID: 1443892
-
A Rare Case of Granulomatous Pneumonitis Due to Intravesical BCG for Bladder Cancer.Acta Med Port. 2019 Apr 30;32(4):316-320. doi: 10.20344/amp.10250. Epub 2019 Apr 30. Acta Med Port. 2019. PMID: 31067427
-
Miliary pulmonary infection after BCG intravesical instillation: a rare, misdiagnosed and mistreated complication.Infez Med. 2017 Dec 1;25(4):366-370. Infez Med. 2017. PMID: 29286018
-
Disseminated Mycobacterium bovis after intravesicular bacillus calmette-Gu rin treatments for bladder cancer.Cancer Control. 2000 Sep-Oct;7(5):476-81. doi: 10.1177/107327480000700512. Cancer Control. 2000. PMID: 11000618 Review. No abstract available.
-
Disseminated Bacillus Calmette-Guérin (BCG) infection with pulmonary and renal involvement: A rare complication of BCG immunotherapy. A case report and narrative review.Pulmonology. 2020 Nov-Dec;26(6):346-352. doi: 10.1016/j.pulmoe.2019.10.001. Epub 2019 Nov 9. Pulmonology. 2020. PMID: 31711964 Review.
Cited by
-
Miliary Tuberculosis that Developed after Intravesical Bacillus Calmette-Guerin Therapy.Intern Med. 2017;56(12):1563-1567. doi: 10.2169/internalmedicine.56.8055. Epub 2017 Jun 15. Intern Med. 2017. PMID: 28626185 Free PMC article.
-
BCG-osis following intravesical BCG treatment leading to miliary pulmonary nodules, penile granulomas and a mycotic aortic aneurysm.BMJ Case Rep. 2016 Jul 14;2016:bcr2016215635. doi: 10.1136/bcr-2016-215635. BMJ Case Rep. 2016. PMID: 27417990 Free PMC article.
References
-
- Morales A, Eidinger D, Bruce AW. Intracavitary bacillus Calmette-Guerin in the treatment of superficial bladder tumors. J Urol 1976;116:180–3 - PubMed
-
- Lamm DL. Efficacy and safety of bacille Calmette-Guérin immunotherapy in superficial bladder cancer. Clin Infect Dis 2000;31(Suppl 3):S86–90 - PubMed
-
- Lamm DL. Comparison of BCG with other intravesical agents. Urology 1991;37(5 Suppl):30–2 - PubMed
-
- Krege S, Giani G, Meyer R, et al. A randomized multicenter trial of adjuvant therapy in superficial bladder cancer: transurethral resection only versus transurethral resection plus mitomycin C versus transurethral resection plus bacillus Calmette-Guerin. Participating clinics . J Urol 1996;156:962–6 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical