

Clinical features and prognosis of patients with coronary spasm-induced non-ST-segment elevation acute coronary syndrome
- PMID: 24811613
- PMCID: PMC4309067
- DOI: 10.1161/JAHA.114.000795
Clinical features and prognosis of patients with coronary spasm-induced non-ST-segment elevation acute coronary syndrome
Abstract
Background: The prevalence, clinical features, and long-term outcome of patients with non-ST-segment elevation acute coronary syndrome (NSTE ACS) associated with coronary spasm are not fully investigated.
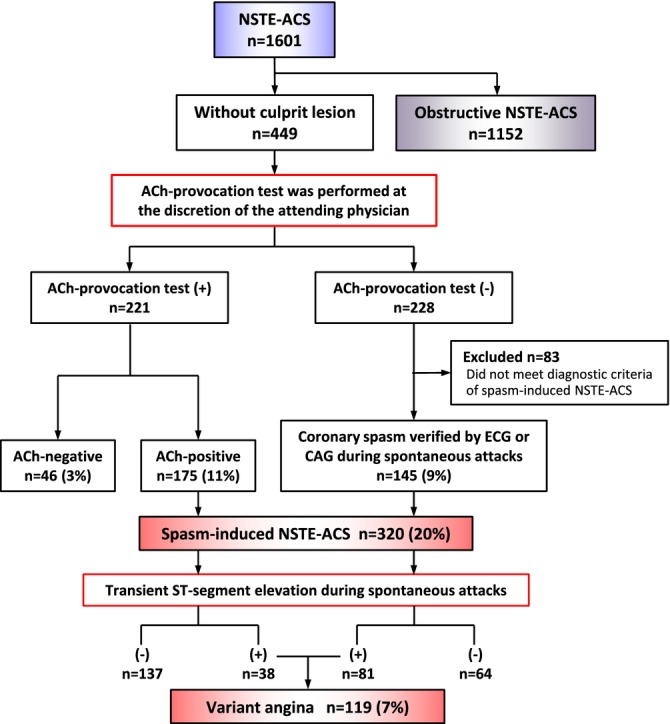
Methods and results: This observational multicenter study enrolled 1601 consecutive patients with suspected NSTE-ACS who underwent cardiac catheterization between January 2001 and December 2010. A culprit lesion was found in 1152 (72%) patients. In patients without a culprit lesion, the acetylcholine provocation test was performed in 221 patients and was positive in 175 patients. In the other patients, coronary spasm was verified in 145 patients during spontaneous attack. Spasm-induced NSTE-ACS was diagnosed in 320 (20%) patients. Multivariable analysis identified age <70 years (odds ratio [OR] 2.19, 95% CI 1.58 to 3.04), estimated glomerular filtration rate >60 mL/min per 1.73 m(2) (OR 1.72, 95% CI 1.16 to 2.56), and lack of hypertension (OR 2.55, 95% CI 1.90 to 3.41), dyslipidemia (OR 2.76, 95% CI 2.05 to 3.73), diabetes mellitus (OR 2.49, 95% CI 1.78 to 3.48), previous myocardial infarction (OR 5.37, 95% CI 2.89 to 10.0), and elevated cardiac biomarkers (OR 2.84, 95% CI 2.11 to 3.83) as significant correlates of spasm-induced NSTE-ACS (P<0.01 for all variables). Transient ST-segment elevation during spontaneous attack (variant angina) was observed in 119 patients with spasm-induced NSTE-ACS. Variant angina was more common in nondyslipidemic men among patients with spasm-induced NSTE-ACS.
Conclusions: The study showed frequent involvement of coronary spasm in the pathogenesis of NSTE-ACS. Variant angina was observed in one third of patients with spasm-induced NSTE-ACS. Coronary spasm should be considered even in patients with less coronary risk factors and nonobstructive coronary arteries.
Keywords: NSTE‐ACS; acetylcholine provocation test; coronary spasm.
Figures
References
-
- Fuster V, Badimon L, Badimon JJ, Chesebro JH. The pathogenesis of coronary artery disease and the acute coronary syndromes (1). N Engl J Med. 1992; 326:242-250. - PubMed
-
- Maseri A, L'Abbate A, Baroldi G, Chierchia S, Marzilli M, Ballestra AM, Severi S, Parodi O, Biagini A, Distante A, Pesola A. Coronary vasospasm as a possible cause of myocardial infarction. A conclusion derived from the study of “preinfarction” angina. N Engl J Med. 1978; 299:1271-1277. - PubMed
-
- DeWood MA, Spores J, Notske R, Mouser LT, Burroughs R, Golden MS, Lang HT. Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N Engl J Med. 1980; 303:897-902. - PubMed
-
- Ong P, Athanasiadis A, Hill S, Vogelsberg H, Voehringer M, Sechtem U. Coronary artery spasm as a frequent cause of acute coronary syndrome: the caspar (coronary artery spasm in patients with acute coronary syndrome) study. J Am Coll Cardiol. 2008; 52:523-527. - PubMed
-
- Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC, Jr, Alpert JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK. ACC/AHA guidelines for the management of patients with ST‐elevation myocardial infarction: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). Circulation. 2004; 110:e82-e292. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
