

Quantitative Magnetic Resonance Imaging UTE-T2* Mapping of Cartilage and Meniscus Healing After Anatomic Anterior Cruciate Ligament Reconstruction
- PMID: 24812196
- PMCID: PMC5278879
- DOI: 10.1177/0363546514532227
Quantitative Magnetic Resonance Imaging UTE-T2* Mapping of Cartilage and Meniscus Healing After Anatomic Anterior Cruciate Ligament Reconstruction
Abstract
Background: An anterior cruciate ligament (ACL) injury greatly increases the risk for premature knee osteoarthritis (OA). Improved diagnosis and staging of early disease are needed to develop strategies to delay or prevent disabling OA.
Purpose: Novel magnetic resonance imaging (MRI) ultrashort echo time (UTE)-T2(*) mapping was evaluated against clinical metrics of cartilage health in cross-sectional and longitudinal studies of human participants before and after ACL reconstruction (ACLR) to show reversible deep subsurface cartilage and meniscus matrix changes.
Study design: Cohort study (diagnosis/prognosis); Level of evidence, 2.
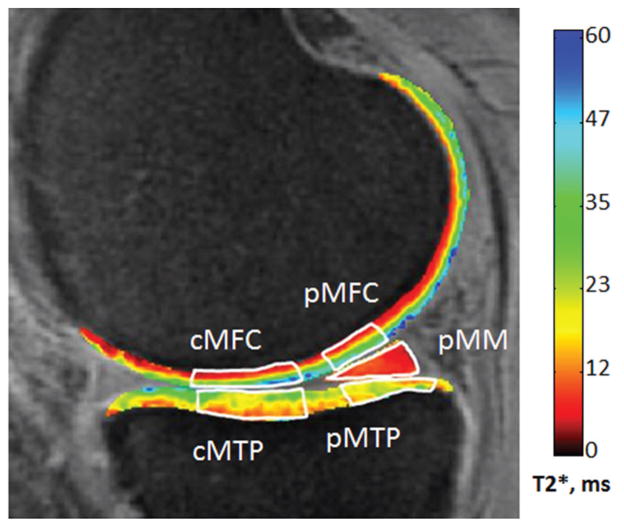
Methods: Forty-two participants (31 undergoing anatomic ACLR; 11 uninjured) underwent 3-T MRI inclusive of a sequence capturing short and ultrashort T2 signals. An arthroscopic examination of the medial meniscus was performed, and modified Outerbridge grades were assigned to the central and posterior medial femoral condyle (cMFC and pMFC, respectively) of ACL-reconstructed patients. Two years after ACLR, 16 patients underwent the same 3-T MRI. UTE-T2(*) maps were generated for the posterior medial meniscus (pMM), cMFC, pMFC, and medial tibial plateau (MTP). Cross-sectional evaluations of UTE-T2(*) and arthroscopic data along with longitudinal analyses of UTE-T2(*) changes were performed.
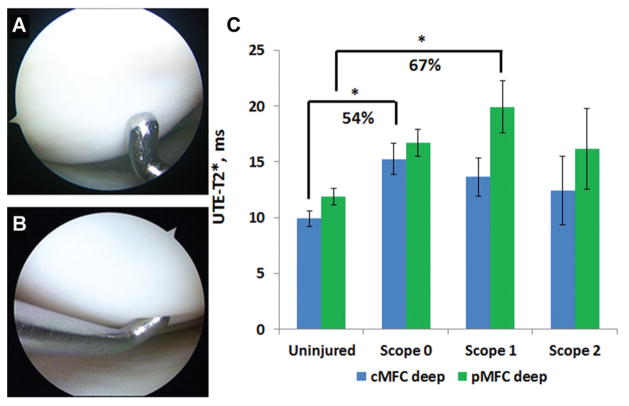
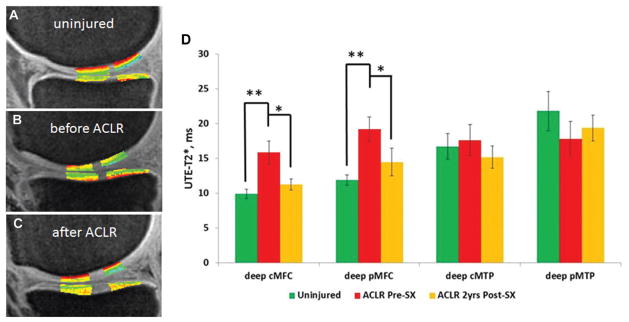
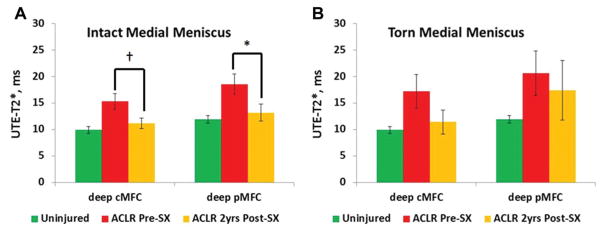
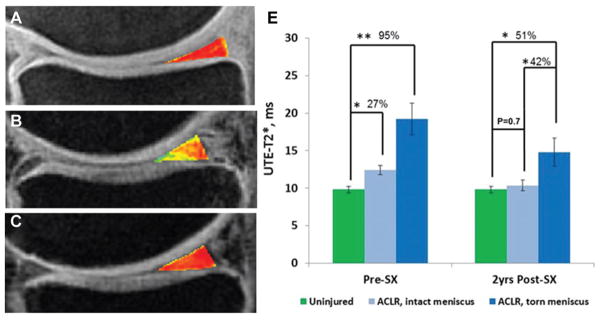
Results: Arthroscopic grades showed that 74% (23/31) of ACL-reconstructed patients had intact cMFC cartilage (Outerbridge grade 0 and 1) and that 90% (28/31) were Outerbridge grade 0 to 2. UTE-T2(*) values in deep cMFC and pMFC cartilage varied significantly with injury status and arthroscopic grade (Outerbridge grade 0-2: n = 39; P = .03 and .04, respectively). Pairwise comparisons showed UTE-T2(*) differences between uninjured controls (n = 11) and patients with arthroscopic Outerbridge grade 0 for the cMFC (n = 12; P = .01) and arthroscopic Outerbridge grade 1 for the pMFC (n = 11; P = .01) only and not individually between arthroscopic Outerbridge grade 0, 1, and 2 of ACL-reconstructed patients (P > .05). Before ACLR, UTE-T2(*) values of deep cMFC and pMFC cartilage of ACL-reconstructed patients were a respective 43% and 46% higher than those of uninjured controls (14.1 ± 5.5 vs 9.9 ± 2.3 milliseconds [cMFC] and 17.4 ± 7.0 vs 11.9 ± 2.4 milliseconds [pMFC], respectively; P = .02 for both). In longitudinal analyses, preoperative elevations in UTE-T2(*) values in deep pMFC cartilage and the pMM in those with clinically intact menisci decreased to levels similar to those in uninjured controls (P = .02 and .005, respectively), suggestive of healing. No decrease in UTE-T2(*) values for the MFC and new elevation in UTE-T2(*) values for the submeniscus MTP were observed in those with meniscus tears.
Conclusion: This study shows that novel UTE-T2(*) mapping demonstrates changes in cartilage deep tissue health according to joint injury status as well as a potential for articular cartilage and menisci to heal deep tissue injuries. Further clinical studies of UTE-T2(*) mapping are needed to determine if it can be used to identify joints at risk for rapid degeneration and to monitor effects of new treatments to delay or prevent the development of OA.
Keywords: ACL reconstruction; MRI; UTE-T2*; anterior cruciate ligament tear; articular cartilage; joint injury; mapping; osteoarthritis; posttraumatic OA; quantitative MRI.
© 2014 The Author(s).
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the National Institutes of Health (R01 AR052784; principal investigator: C.R.C.). Y.Q. has a patent on the acquisition-weighted stack of spirals imaging method.
Figures
References
-
- Adams ME, Brandt KD. Hypertrophic repair of canine articular cartilage in osteoarthritis after anterior cruciate ligament transection. J Rheumatol. 1991;18(3):428–435. - PubMed
-
- Akella SV, Regatte RR, Gougoutas AJ, et al. Proteoglycan-induced changes in T1rho-relaxation of articular cartilage at 4T. Magn Reson Med. 2001;46(3):419–423. - PubMed
-
- Bashir A, Gray ML, Hartke J, Burstein D. Nondestructive imaging of human cartilage glycosaminoglycan concentration by MRI. Magn Reson Med. 1999;41(5):857–865. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
