

Abdominal aortic calcium, coronary artery calcium, and cardiovascular morbidity and mortality in the Multi-Ethnic Study of Atherosclerosis
- PMID: 24812323
- PMCID: PMC4153597
- DOI: 10.1161/ATVBAHA.114.303268
Abdominal aortic calcium, coronary artery calcium, and cardiovascular morbidity and mortality in the Multi-Ethnic Study of Atherosclerosis
Erratum in
-
Correction.Arterioscler Thromb Vasc Biol. 2015 Jan;35(1):e1. doi: 10.1161/ATV.0000000000000014. Arterioscler Thromb Vasc Biol. 2015. PMID: 30525947 No abstract available.
Abstract
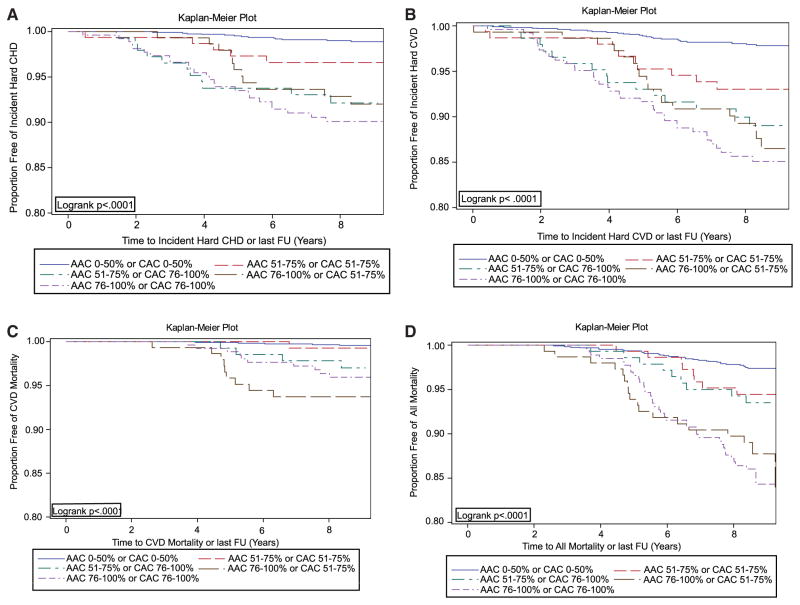
Objective: To evaluate the predictive value of abdominal aortic calcium (AAC) for incident cardiovascular disease (CVD) independent of coronary artery calcium (CAC).
Approach and results: We evaluated the association of AAC with CVD in 1974 men and women aged 45 to 84 years randomly selected from the Multi-Ethnic Study of Atherosclerosis participants who had complete AAC and CAC data from computed tomographic scans. AAC and CAC were each divided into following 3 percentile categories: 0 to 50th, 51st to 75th, and 76th to 100th. During a mean of 5.5 years of follow-up, there were 50 hard coronary heart disease events, 83 hard CVD events, 30 fatal CVD events, and 105 total deaths. In multivariable-adjusted Cox models including both AAC and CAC, comparing the fourth quartile with the ≤ 50th percentile, AAC and CAC were each significantly and independently predictive of hard coronary heart disease and hard CVD, with hazard ratios ranging from 2.4 to 4.4. For CVD mortality, the hazard ratio was highly significant for the fourth quartile of AAC, 5.9 (P=0.01), whereas the association for the fourth quartile of CAC (hazard ratio, 2.1) was not significant. For total mortality, the fourth quartile hazard ratio for AAC was 2.7 (P=0.001), and for CAC, it was 1.9, P=0.04. Area under the receiver operating characteristic curve analyses showed improvement for both AAC and CAC separately, although improvement was greater with CAC for hard coronary heart disease and hard CVD, and greater with AAC for CVD mortality and total mortality. Sensitivity analyses defining AAC and CAC as continuous variables mirrored these results.
Conclusions: AAC and CAC predicted hard coronary heart disease and hard CVD events independent of one another. Only AAC was independently related to CVD mortality, and AAC showed a stronger association than CAC with total mortality.
Keywords: aortic diseases; calcium; cardiovascular diseases; diagnostic imaging; epidemiology.
© 2014 American Heart Association, Inc.
Conflict of interest statement
N. Wong is a Consultant (significant) at Re-Engineering Healthcare, Inc. The other authors report no conflicts.
Figures
Similar articles
-
Greater Volume but not Higher Density of Abdominal Aortic Calcium Is Associated With Increased Cardiovascular Disease Risk: MESA (Multi-Ethnic Study of Atherosclerosis).Circ Cardiovasc Imaging. 2016 Nov;9(11):e005138. doi: 10.1161/CIRCIMAGING.116.005138. Circ Cardiovasc Imaging. 2016. PMID: 27903540 Free PMC article.
-
Abdominal Compared With Coronary Artery Calcification and Incident Cardiovascular Events and Mortality in Black Adults.Circ Cardiovasc Imaging. 2024 Dec;17(12):e016775. doi: 10.1161/CIRCIMAGING.124.016775. Epub 2024 Nov 27. Circ Cardiovasc Imaging. 2024. PMID: 39601135
-
Cardiovascular Event Prediction and Risk Reclassification by Coronary, Aortic, and Valvular Calcification in the Framingham Heart Study.J Am Heart Assoc. 2016 Feb 22;5(2):e003144. doi: 10.1161/JAHA.115.003144. J Am Heart Assoc. 2016. PMID: 26903006 Free PMC article.
-
Computed tomography-derived cardiovascular risk markers, incident cardiovascular events, and all-cause mortality in nondiabetics: the Multi-Ethnic Study of Atherosclerosis.Eur J Prev Cardiol. 2014 Oct;21(10):1233-41. doi: 10.1177/2047487313492065. Epub 2013 May 20. Eur J Prev Cardiol. 2014. PMID: 23689526 Free PMC article.
-
Peripheral Artery Disease and Aortic Disease.Glob Heart. 2016 Sep;11(3):313-326. doi: 10.1016/j.gheart.2016.08.005. Glob Heart. 2016. PMID: 27741978 Free PMC article. Review.
Cited by
-
Gender-specific correlations between remnant cholesterol and severe abdominal aortic calcification in American adults.Front Endocrinol (Lausanne). 2024 Sep 16;15:1415424. doi: 10.3389/fendo.2024.1415424. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39351538 Free PMC article.
-
Association between urinary biomarkers of polycyclic aromatic hydrocarbons and severe abdominal aortic calcification in adults: data from the National Health and Examination Nutrition Survey.BMC Cardiovasc Disord. 2023 Feb 23;23(1):104. doi: 10.1186/s12872-023-03122-0. BMC Cardiovasc Disord. 2023. PMID: 36823527 Free PMC article.
-
Associations of cardiovascular disease risk factors with abdominal aortic calcium volume and density: The Multi-Ethnic Study of Atherosclerosis (MESA).Atherosclerosis. 2016 Dec;255:54-58. doi: 10.1016/j.atherosclerosis.2016.10.036. Epub 2016 Oct 20. Atherosclerosis. 2016. PMID: 27816809 Free PMC article.
-
Association between a body shape index and cognitive impairment among US older adults aged 40 years and above from a cross-sectional survey of the NHANES 2011-2014.Front Endocrinol (Lausanne). 2024 Sep 23;15:1411701. doi: 10.3389/fendo.2024.1411701. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39377074 Free PMC article.
-
Abdominal aortic calcification (AAC) and ankle-brachial index (ABI) predict health care costs and utilization in older men, independent of prevalent clinical cardiovascular disease and each other.Atherosclerosis. 2020 Feb;295:31-37. doi: 10.1016/j.atherosclerosis.2020.01.012. Epub 2020 Jan 19. Atherosclerosis. 2020. PMID: 32000096 Free PMC article.
References
-
- Assmann G, Cullen P, Schulte H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Münster (PROCAM) study. Circulation. 2002;105:310–315. - PubMed
-
- D’Agostino RB, Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117:743–753. - PubMed
-
- Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007;297:611–619. - PubMed
-
- Folsom AR, Kronmal RA, Detrano RC, O’Leary DH, Bild DE, Bluemke DA, Budoff MJ, Liu K, Shea S, Szklo M, Tracy RP, Watson KE, Burke GL. Coronary artery calcification compared with carotid intima-media thickness in the prediction of cardiovascular disease incidence: the Multi-Ethnic Study of Atherosclerosis (MESA) Arch Intern Med. 2008;168:1333–1339. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
