

Caval-aortic access to allow transcatheter aortic valve replacement in otherwise ineligible patients: initial human experience
- PMID: 24814495
- PMCID: PMC4105161
- DOI: 10.1016/j.jacc.2014.04.015
Caval-aortic access to allow transcatheter aortic valve replacement in otherwise ineligible patients: initial human experience
Abstract
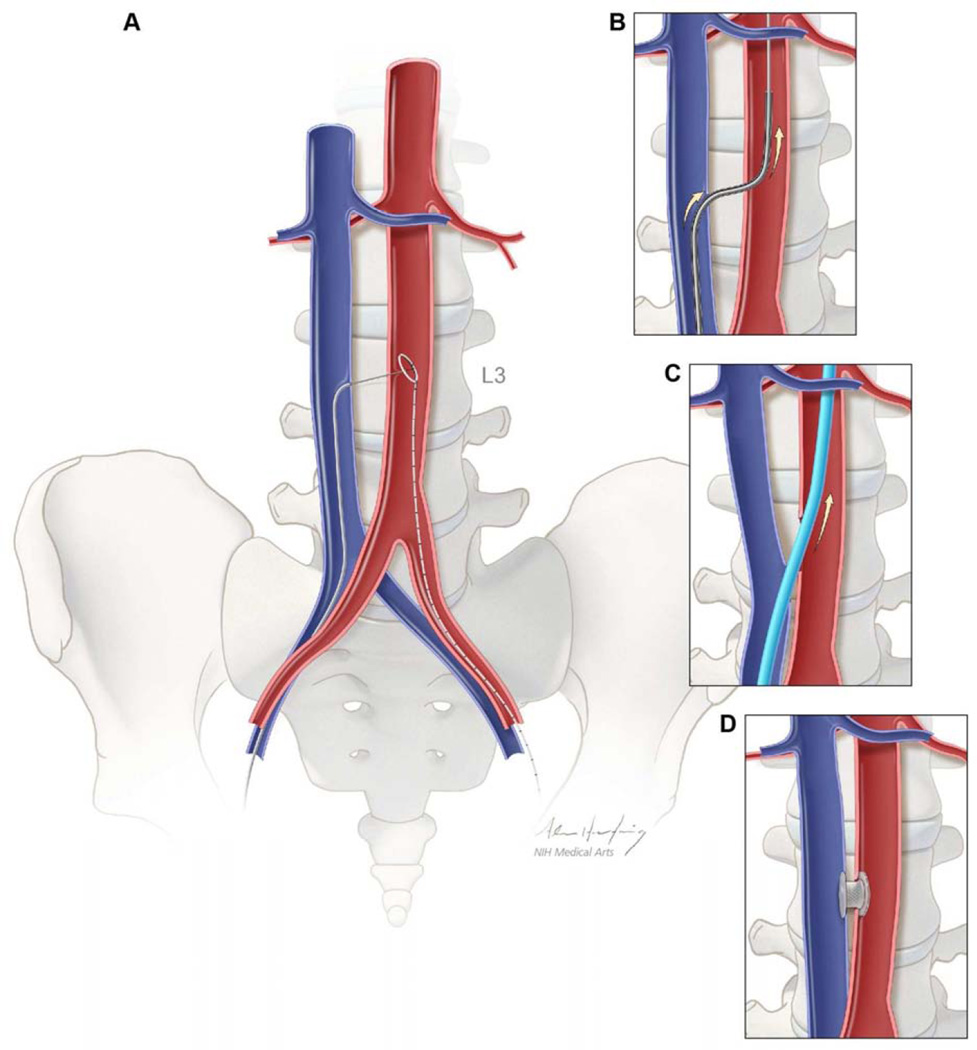
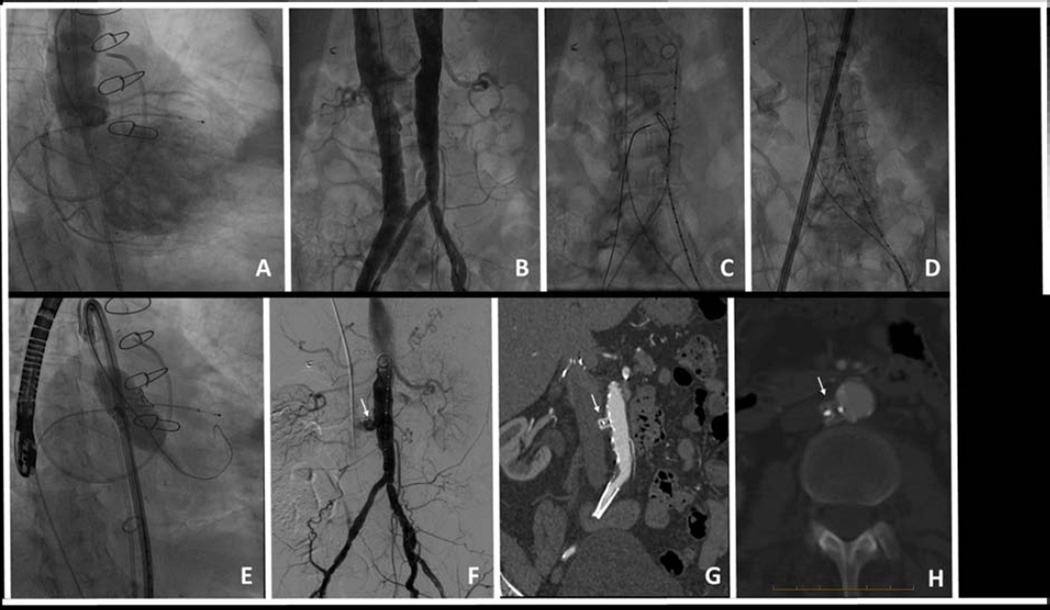
Objectives: This study describes the first use of caval-aortic access and closure to enable transcatheter aortic valve replacement (TAVR) in patients who lacked other access options. Caval-aortic access refers to percutaneous entry into the abdominal aorta from the femoral vein through the adjoining inferior vena cava.
Background: TAVR is attractive in high-risk or inoperable patients with severe aortic stenosis. Available transcatheter valves require large introducer sheaths, which are a risk for major vascular complications or preclude TAVR altogether. Caval-aortic access has been successful in animals.
Methods: We performed a single-center retrospective review of procedural and 30-day outcomes of prohibitive-risk patients who underwent TAVR via caval-aortic access.
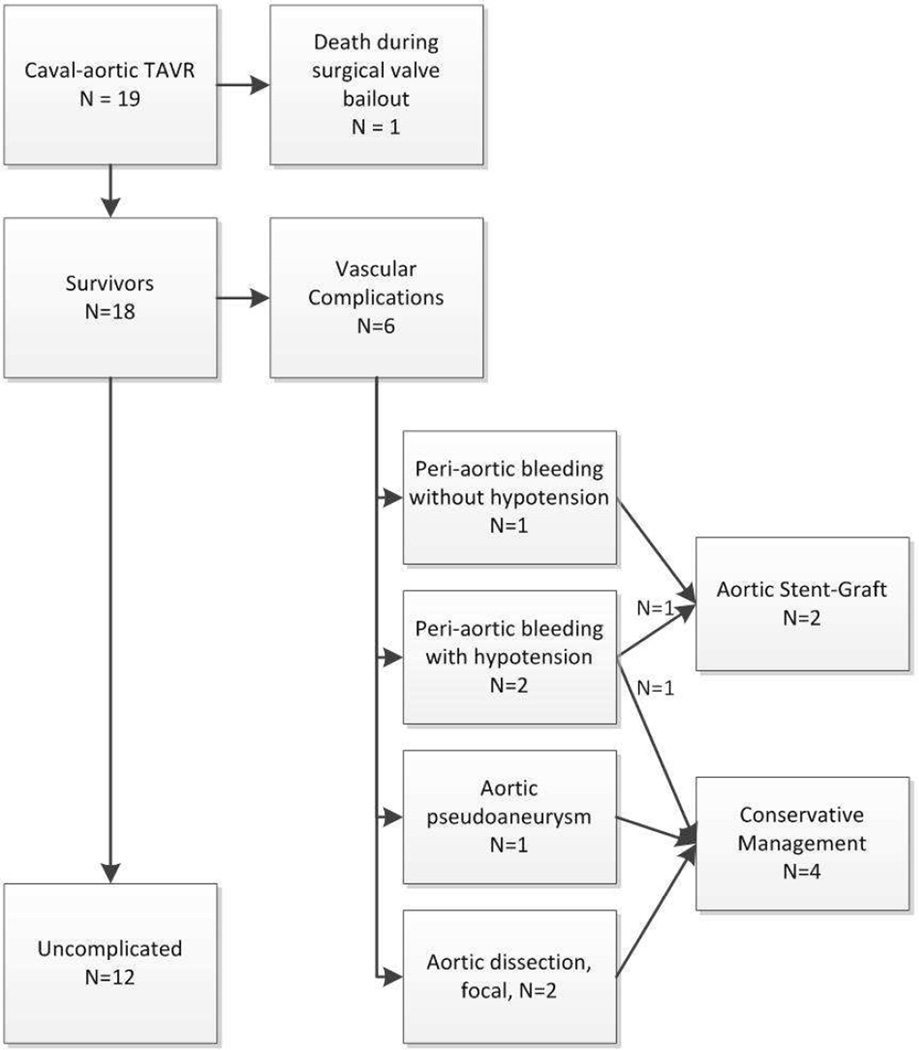
Results: Between July 2013 and January 2014, 19 patients underwent TAVR via caval-aortic access; 79% were women. Caval-aortic access and tract closure were successful in all 19 patients; TAVR was successful in 17 patients. Six patients experienced modified VARC-2 major vascular complications, 2 (11%) of whom required intervention. Most (79%) required blood transfusion. There were no deaths attributable to caval-aortic access. Throughout the 111 (range 39 to 229) days of follow up, there were no post-discharge complications related to tract creation or closure. All patients had persistent aorto-caval flow immediately post-procedure. Of the 16 patients who underwent repeat imaging after the first week, 15 (94%) had complete closure of the residual aorto-caval tract.
Conclusions: Percutaneous transcaval venous access to the aorta allows TAVR in otherwise ineligible patients, and may offer a new access strategy for other applications requiring large transcatheter implants.
Keywords: caval-aortic; extra-anatomic procedures; transcatheter aortic valve replacement; transcaval.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Percutaneous access, no matter what!J Am Coll Cardiol. 2015 Jan 27;65(3):309-10. doi: 10.1016/j.jacc.2014.09.085. J Am Coll Cardiol. 2015. PMID: 25614431 No abstract available.
-
Reply: percutaneous access, no matter what!J Am Coll Cardiol. 2015 Jan 27;65(3):310-1. doi: 10.1016/j.jacc.2014.10.038. J Am Coll Cardiol. 2015. PMID: 25614432 Free PMC article. No abstract available.
References
-
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. The New England journal of medicine. 2010;363:1597–1607. - PubMed
-
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. The New England journal of medicine. 2011;364:2187–2198. - PubMed
-
- Blanke P, Euringer W, Baumann T, et al. Combined assessment of aortic root anatomy and aortoiliac vasculature with dual-source CT as a screening tool in patients evaluated for transcatheter aortic valve implantation. AJR American journal of roentgenology. 2010;195:872–881. - PubMed
-
- Babcock MJ, Lavine S, Strom JA, Bass TA, Guzman LA. Candidates for transcatheter aortic valve replacement: Fitting the PARTNERS criteria. Catheter Cardiovasc Interv. 2013;82:655–661. - PubMed
-
- Genereux P, Webb JG, Svensson LG, et al. Vascular complications after transcatheter aortic valve replacement: insights from the PARTNER trial. J Am Coll Cardiol. 2012;60:1043–1052. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
