

Hospital-acquired Clostridium difficile infections: estimating all-cause mortality and length of stay
- PMID: 24815305
- PMCID: PMC4224274
- DOI: 10.1097/EDE.0000000000000119
Hospital-acquired Clostridium difficile infections: estimating all-cause mortality and length of stay
Abstract
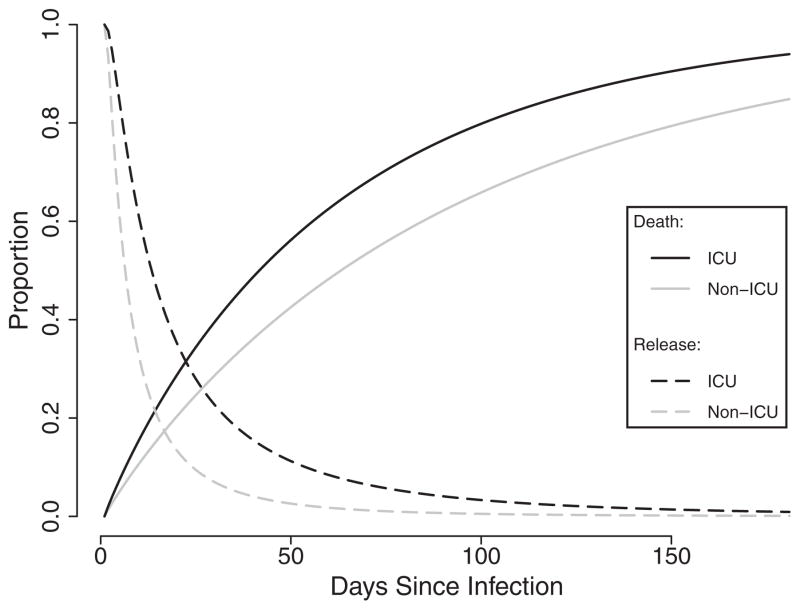
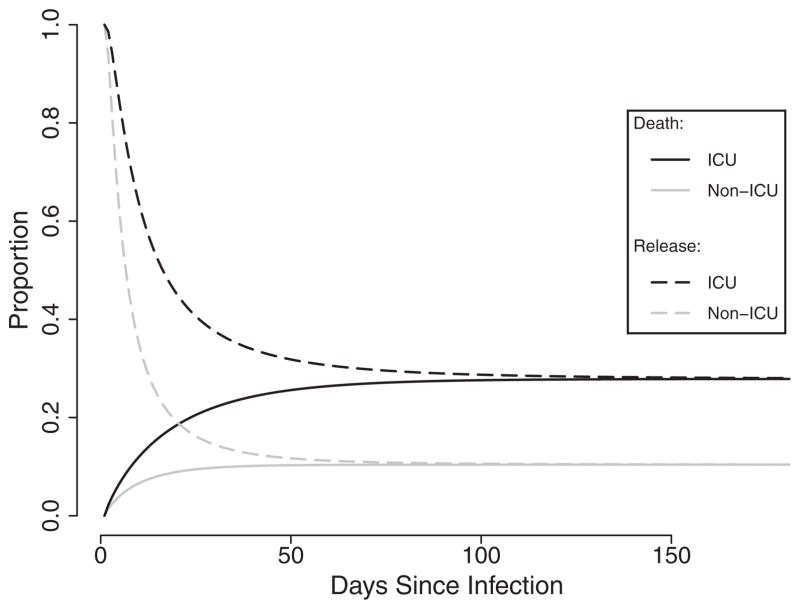
Background: Clostridium difficile is a health care-associated infection of increasing importance. The purpose of this study was to estimate the time until death from any cause and time until release among patients with C. difficile, comparing the burden of those in the intensive care unit (ICU) with those in the general hospital population.
Methods: A parametric mixture model was used to estimate event times, as well as the case-fatality ratio in ICU and non-ICU patients within a cohort of 609 adult incident cases of C. difficile in the Southeastern United States between 1 July 2009 and 31 December 2010.
Results: ICU patients had twice the median time to death (relative time = 1.97 [95% confidence interval (CI) = 0.96-4.01]) and nearly twice the median time to release (1.88 [1.40-2.51]) compared with non-ICU patients. ICU patients also experienced 3.4 times the odds of mortality (95% CI = 1.8-6.2). Cause-specific competing risks analysis underestimated the relative survival time until death (0.65 [0.36-1.17]) compared with the mixture model.
Conclusions: Patients with C. difficile in the ICU experienced higher mortality and longer lengths of stay within the hospital. ICU patients with C. difficile infection represent a population in need of particular attention, both to prevent adverse patient outcomes and to minimize transmission of C. difficile to other hospitalized patients.
Figures
References
-
- HCUPnet. [Accessed 17 September 2012];Agency for Healthcare Research and Quality. 2006 Available at: http://hcupnet.ahrq.gov/
-
- Ghantoji SS, Sail K, Lairson DR, DuPont HL, Garey KW. Economic healthcare costs of Clostridium difficile infection: a systematic review. J Hosp Infect. 2010;74:309–318. - PubMed
-
- Miller BA, Chen LF, Sexton DJ, Anderson DJ. Comparison of the burdens of hospital-onset, healthcare facility-associated Clostridium difficile Infection and of healthcare-associated infection due to methicillin-resistant Staphylococcus aureus in community hospitals. Infect Control Hosp Epidemiol. 2011;32:387–390. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
