

Development and validation of insulin-like growth factor-1 score to assess hepatic reserve in hepatocellular carcinoma
- PMID: 24815863
- PMCID: PMC4085880
- DOI: 10.1093/jnci/dju088
Development and validation of insulin-like growth factor-1 score to assess hepatic reserve in hepatocellular carcinoma
Abstract
Background: Child-Turcotte-Pugh (CTP) score is the standard tool to assess hepatic reserve in hepatocellular carcinoma (HCC), and CTP-A is the classic group for active therapy. However, CTP stratification accuracy has been questioned. We hypothesized that plasma insulin-like growth factor 1 (IGF-1) is a valid surrogate for hepatic reserve to replace the subjective parameters in CTP score to improve its prognostic accuracy.
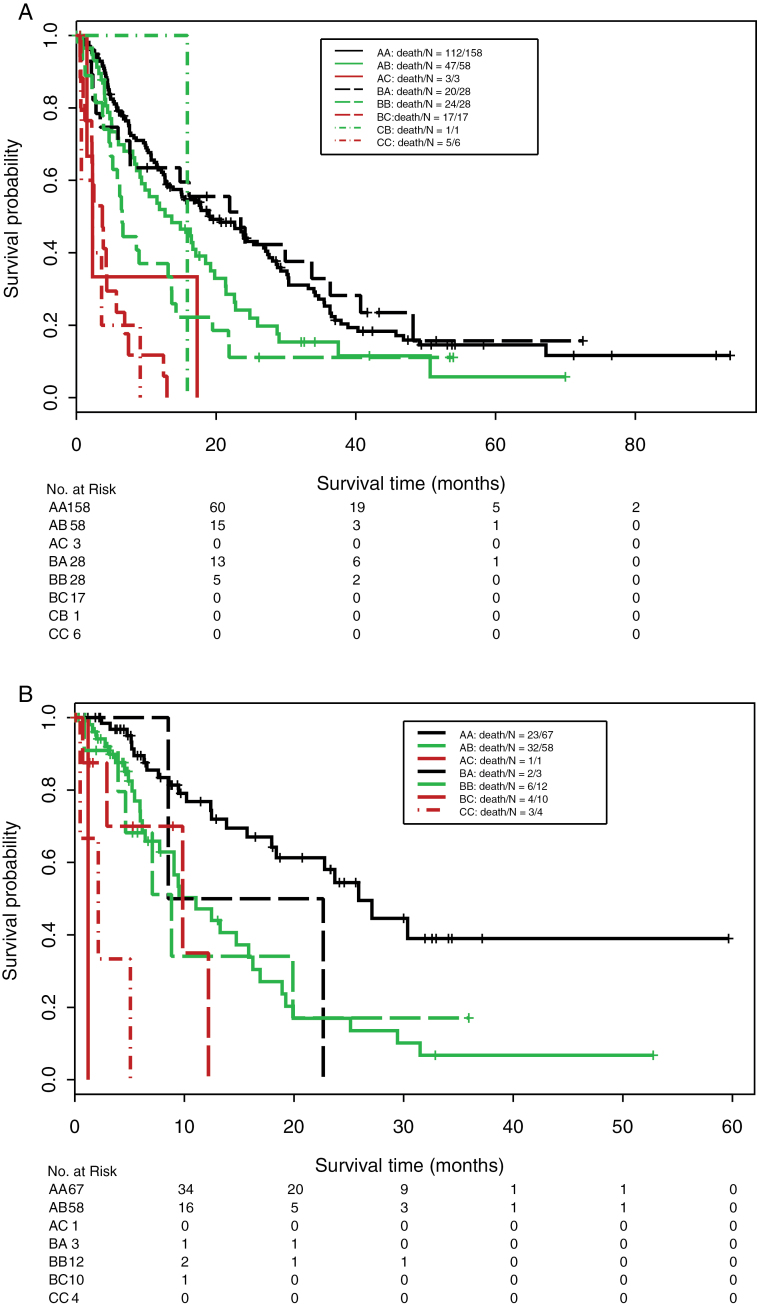
Methods: We retrospectively tested plasma IGF-1 levels in the training set (n = 310) from MD Anderson Cancer Center. Recursive partitioning identified three optimal IGF-1 ranges that correlated with overall survival (OS): greater than 50 ng/mL = 1 point; 26 to 50 ng/mL = 2 points; and less than 26 ng/mL = 3 points. We modified the CTP score by replacing ascites and encephalopathy grading with plasma IGF-1 value (IGF-CTP) and subjected both scores to log-rank analysis. Harrell's C-index and U-statistics were used to compare the prognostic performance of both scores in both the training and validation cohorts (n = 155). All statistical tests were two-sided.
Results: Patients' stratification was statistically significantly stronger for IGF-CTP than CTP score for the training (P = .003) and the validation cohort (P = .005). Patients reclassified by IGF-CTP relative to their original CTP score were better stratified by their new risk groups. Most important, patients classified as A by CTP but B by IGF-CTP had statistically significantly worse OS than those who remained under class A by IGF-CTP in both cohorts (P = .03 and P < .001, respectively, from Cox regression models). AB patients had a worse OS than AA patients in both the training and validation set (hazard ratio [HR] = 1.45, 95% confidence interval [CI] = 1.03 to 2.04, P = .03; HR = 2.83, 95% CI = 1.65 to 4.85, P < .001, respectively).
Conclusions: The IGF-CTP score is simple, blood-based, and cost-effective, stratified HCC better than CTP score, and validated well on two independent cohorts. International validation studies are warranted.
© The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Child CG. Remote results of portal surgery in liver cirrhosis. Rev Int Hepatol. 1964;14:287–288 - PubMed
-
- Pugh RN, Murray-Lyon IM, Dawson JL, et al. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646–649 - PubMed
-
- Llovet JM, Di Bisceglie AM, Bruix J, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008;100(10):698–711 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
