

Coronary responses to cold air inhalation following afferent and efferent blockade
- PMID: 24816257
- PMCID: PMC4101647
- DOI: 10.1152/ajpheart.00174.2014
Coronary responses to cold air inhalation following afferent and efferent blockade
Abstract
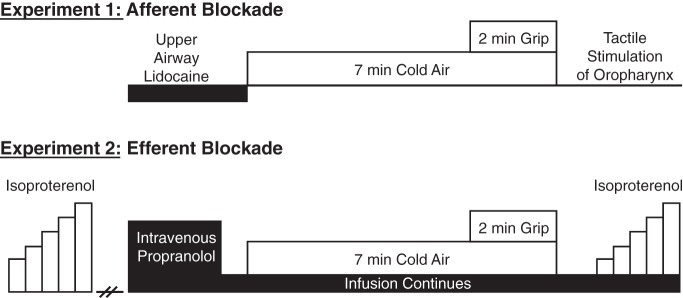
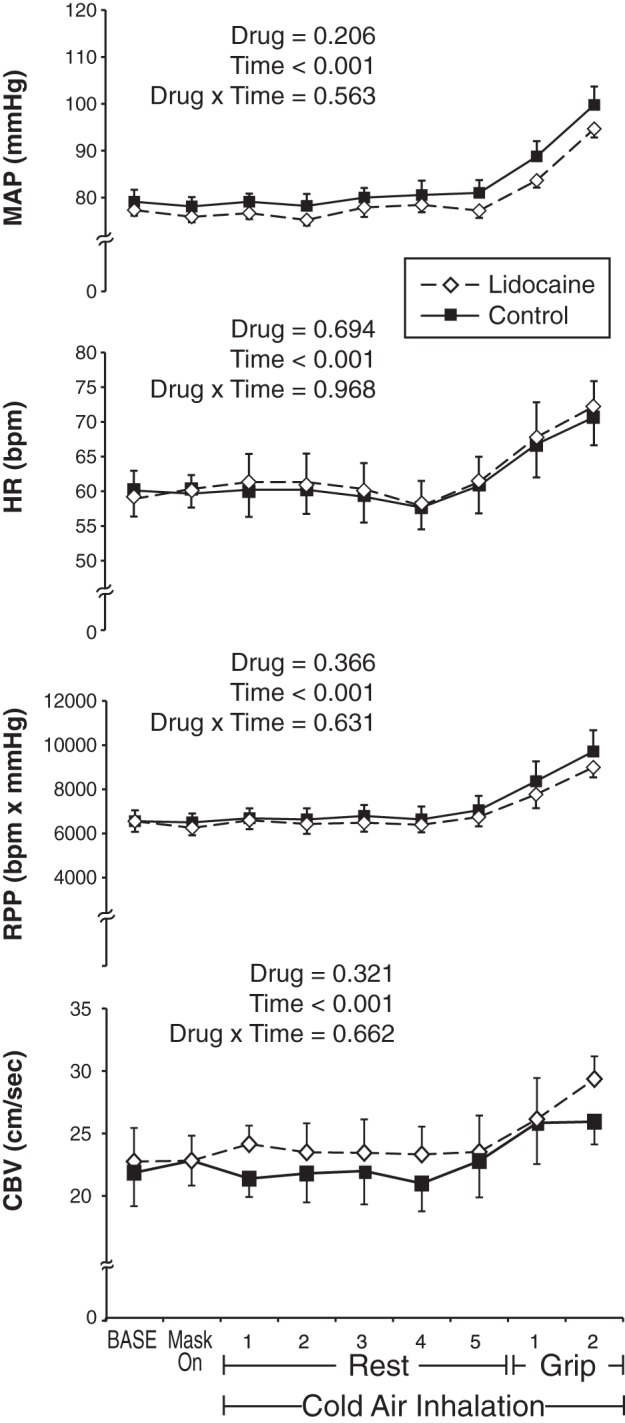
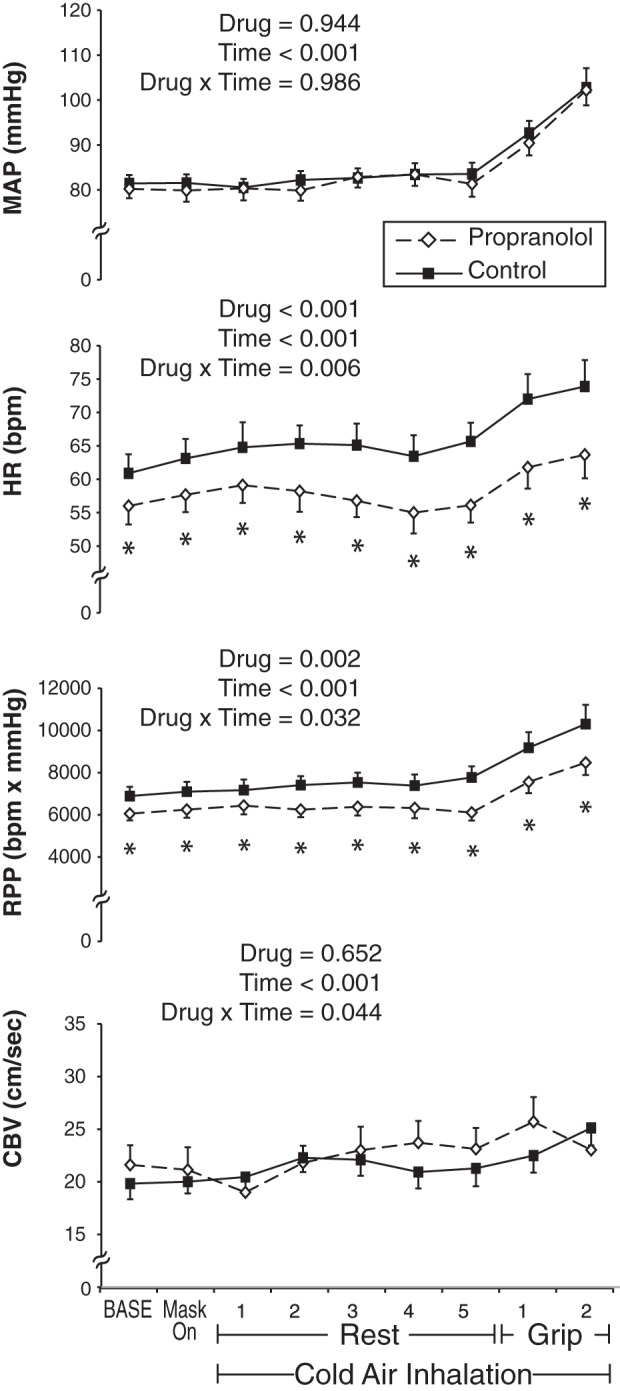
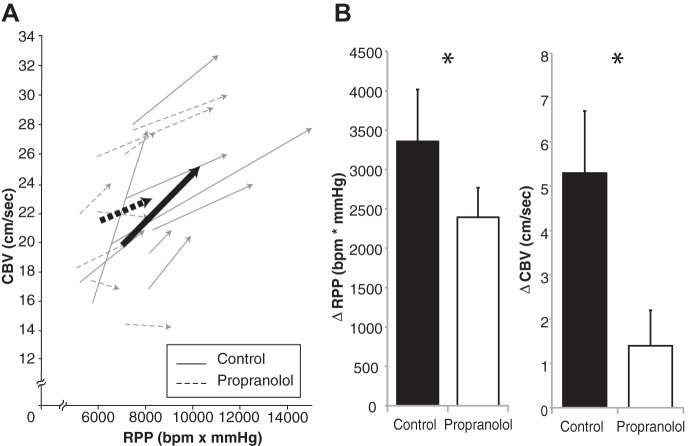
Cardiac ischemia and angina pectoris are commonly experienced during exertion in a cold environment. In the current study we tested the hypotheses that oropharyngeal afferent blockade (i.e., local anesthesia of the upper airway with lidocaine) as well as systemic β-adrenergic receptor blockade (i.e., intravenous propranolol) would improve the balance between myocardial oxygen supply and demand in response to the combined stimulus of cold air inhalation (-15 to -30°C) and isometric handgrip exercise (Cold + Grip). Young healthy subjects underwent Cold + Grip following lidocaine, propranolol, and control (no drug). Heart rate, blood pressure, and coronary blood flow velocity (CBV, from Doppler echocardiography) were continuously measured. Rate-pressure product (RPP) was calculated, and changes from baseline were compared between treatments. The change in RPP at the end of Cold + Grip was not different between lidocaine (2,441 ± 376) and control conditions (3,159 ± 626); CBV responses were also not different between treatments. With propranolol, heart rate (8 ± 1 vs. 14 ± 3 beats/min) and RPP responses to Cold + Grip were significantly attenuated. However, at peak exercise propranolol also resulted in a smaller ΔCBV (1.4 ± 0.8 vs. 5.3 ± 1.4 cm/s, P = 0.035), such that the relationship between coronary flow and cardiac metabolism was impaired under propranolol (0.43 ± 0.37 vs. 2.1 ± 0.63 arbitrary units). These data suggest that cold air breathing and isometric exercise significantly influence efferent control of coronary blood flow. Additionally, β-adrenergic vasodilation may play a significant role in coronary regulation during exercise.
Keywords: blood pressure; heart rate; lidocaine; oropharynx; propranolol; vascular resistance.
Copyright © 2014 the American Physiological Society.
Figures
Similar articles
-
β-Adrenergic receptor blockade impairs coronary exercise hyperemia in young men but not older men.Am J Physiol Heart Circ Physiol. 2014 Nov 15;307(10):H1497-503. doi: 10.1152/ajpheart.00584.2014. Epub 2014 Sep 19. Am J Physiol Heart Circ Physiol. 2014. PMID: 25239806 Free PMC article. Clinical Trial.
-
Beta-1 vs. beta-2 adrenergic control of coronary blood flow during isometric handgrip exercise in humans.J Appl Physiol (1985). 2017 Aug 1;123(2):337-343. doi: 10.1152/japplphysiol.00106.2017. Epub 2017 Jun 1. J Appl Physiol (1985). 2017. PMID: 28572492 Free PMC article. Clinical Trial.
-
Effect of cold air inhalation and isometric exercise on coronary blood flow and myocardial function in humans.J Appl Physiol (1985). 2011 Dec;111(6):1694-702. doi: 10.1152/japplphysiol.00909.2011. Epub 2011 Sep 22. J Appl Physiol (1985). 2011. PMID: 21940852 Free PMC article.
-
Aging attenuates the coronary blood flow response to cold air breathing and isometric handgrip in healthy humans.Am J Physiol Heart Circ Physiol. 2012 Apr 15;302(8):H1737-46. doi: 10.1152/ajpheart.01195.2011. Epub 2012 Feb 17. Am J Physiol Heart Circ Physiol. 2012. PMID: 22345567 Free PMC article.
-
Regulation of coronary blood flow during exercise.Physiol Rev. 2008 Jul;88(3):1009-86. doi: 10.1152/physrev.00045.2006. Physiol Rev. 2008. PMID: 18626066 Review.
Cited by
-
Effects of alpha-adrenergic receptor blockade on coronary circulation in postmenopausal women.Eur J Appl Physiol. 2023 Dec;123(12):2779-2790. doi: 10.1007/s00421-023-05267-4. Epub 2023 Jun 27. Eur J Appl Physiol. 2023. PMID: 37368136
-
Peripheral revascularization attenuates the exercise pressor reflex and increases coronary exercise hyperemia in peripheral arterial disease.J Appl Physiol (1985). 2018 Jul 1;125(1):58-63. doi: 10.1152/japplphysiol.01046.2017. Epub 2018 Apr 12. J Appl Physiol (1985). 2018. PMID: 29648515 Free PMC article.
-
β-Adrenergic receptor blockade impairs coronary exercise hyperemia in young men but not older men.Am J Physiol Heart Circ Physiol. 2014 Nov 15;307(10):H1497-503. doi: 10.1152/ajpheart.00584.2014. Epub 2014 Sep 19. Am J Physiol Heart Circ Physiol. 2014. PMID: 25239806 Free PMC article. Clinical Trial.
-
Effect of adrenergic agonists on coronary blood flow: a laboratory study in healthy volunteers.Physiol Rep. 2016 May;4(10):e12806. doi: 10.14814/phy2.12806. Physiol Rep. 2016. PMID: 27225628 Free PMC article.
-
Cardiovascular diseases, cold exposure and exercise.Temperature (Austin). 2018 Feb 1;5(2):123-146. doi: 10.1080/23328940.2017.1414014. eCollection 2018. Temperature (Austin). 2018. PMID: 30377633 Free PMC article. Review.
References
-
- Barbato E. Role of adrenergic receptors in human coronary vasomotion. Heart 95: 603–608, 2009 - PubMed
-
- Baumgart D, Haude M, Gorge G, Liu F, Ge J, Grosse-Eggebrecht C, Erbel R, Heusch G. Augmented alpha-adrenergic constriction of atherosclerotic human coronary arteries. Circulation 99: 2090–2097, 1999 - PubMed
-
- Bell C, Seals DR, Monroe MB, Day DS, Shapiro LF, Johnson DG, Jones PP. Tonic sympathetic support of metabolic rate is attenuated with age, sedentary lifestyle, and female sex in healthy adults. J Clin Endocrinol Metab 86: 4440–4444, 2001 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources