

Infliximab therapy increases the frequency of circulating CD16(+) monocytes and modifies macrophage cytokine response to bacterial infection
- PMID: 24816497
- PMCID: PMC4137855
- DOI: 10.1111/cei.12375
Infliximab therapy increases the frequency of circulating CD16(+) monocytes and modifies macrophage cytokine response to bacterial infection
Abstract
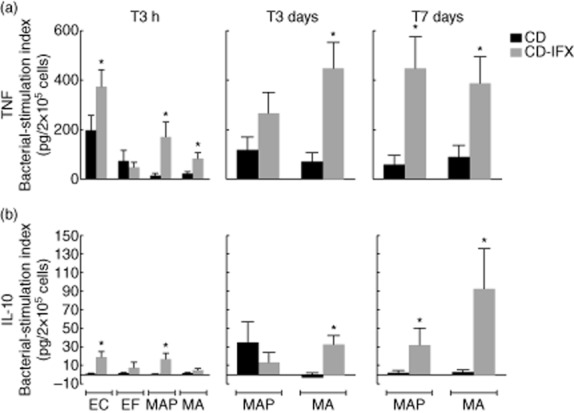
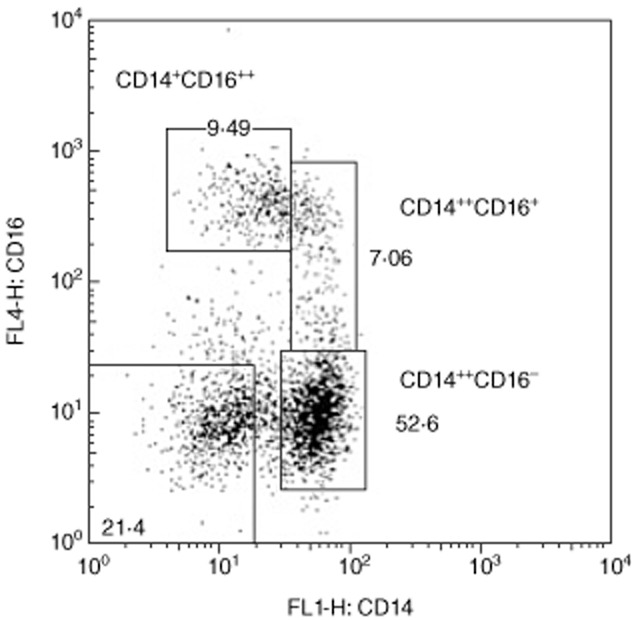
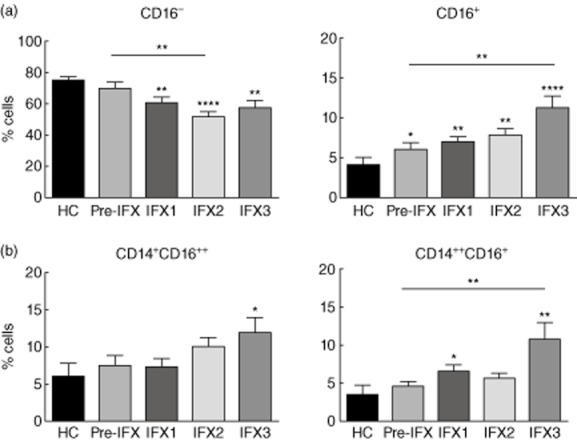
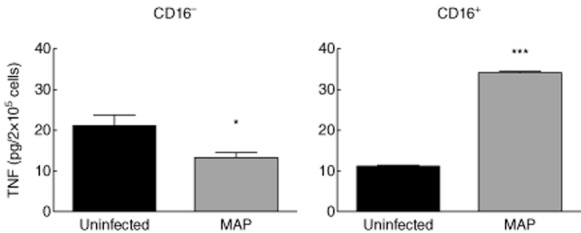
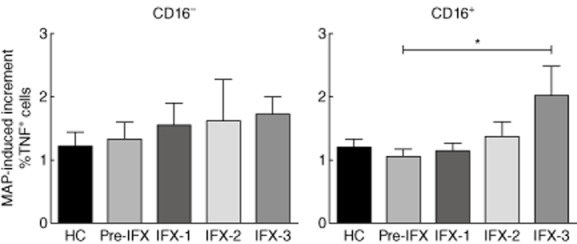
Crohn's disease (CD) has been correlated with altered macrophage response to microorganisms. Considering the efficacy of infliximab treatment on CD remission, we investigated infliximab effects on circulating monocyte subsets and on macrophage cytokine response to bacteria. Human peripheral blood monocyte-derived macrophages were obtained from CD patients, treated or not with infliximab. Macrophages were infected with Escherichia coli, Enterococcus faecalis, Mycobacterium avium subsp. paratuberculosis (MAP) or M. avium subsp avium, and cytokine levels [tumour necrosis factor (TNF) and interleukin (IL)-10] were evaluated at different time-points. To evaluate infliximab-dependent effects on monocyte subsets, we studied CD14 and CD16 expression by peripheral blood monocytes before and after different infliximab administrations. We also investigated TNF secretion by macrophages obtained from CD16(+) and CD16(-) monocytes and the frequency of TNF(+) cells among CD16(+) and CD16(-) monocyte-derived macrophages from CD patients. Infliximab treatment resulted in elevated TNF and IL-10 macrophage response to bacteria. An infliximab-dependent increase in the frequency of circulating CD16(+) monocytes (particularly the CD14(++) CD16(+) subset) was also observed (before infliximab: 4·65 ± 0·58%; after three administrations: 10·68 ± 2·23%). In response to MAP infection, macrophages obtained from CD16(+) monocytes were higher TNF producers and CD16(+) macrophages from infliximab-treated CD patients showed increased frequency of TNF(+) cells. In conclusion, infliximab treatment increased the TNF production of CD macrophages in response to bacteria, which seemed to depend upon enrichment of CD16(+) circulating monocytes, particularly of the CD14(++) CD16(+) subset. Infliximab treatment of CD patients also resulted in increased macrophage IL-10 production in response to bacteria, suggesting an infliximab-induced shift to M2 macrophages.
Keywords: cytokine secretion; inflammatory bowel diseases; infliximab therapy; macrophages; monocyte subsets.
© 2014 British Society for Immunology.
Figures
Similar articles
-
Macrophages from IBD patients exhibit defective tumour necrosis factor-α secretion but otherwise normal or augmented pro-inflammatory responses to infection.Immunobiology. 2011 Aug;216(8):961-70. doi: 10.1016/j.imbio.2011.01.002. Epub 2011 Jan 12. Immunobiology. 2011. PMID: 21269730
-
Crohn's Disease Patients with Depression Exhibit Alterations in Monocyte/Macrophage Phenotype and Increased Proinflammatory Cytokine Production.Dig Dis. 2020;38(3):211-221. doi: 10.1159/000501122. Epub 2019 Jun 19. Dig Dis. 2020. PMID: 31216541
-
Expression of Toll-like receptor 2 on CD16+ blood monocytes and synovial tissue macrophages in rheumatoid arthritis.Arthritis Rheum. 2004 May;50(5):1457-67. doi: 10.1002/art.20219. Arthritis Rheum. 2004. PMID: 15146415
-
Transcending conventional therapies: the role of biologic and other novel therapies.Inflamm Bowel Dis. 2001 May;7 Suppl 1:S9-16. doi: 10.1002/ibd.3780070504. Inflamm Bowel Dis. 2001. PMID: 11380043 Review.
-
Monocytes mediate HIV neuropathogenesis: mechanisms that contribute to HIV associated neurocognitive disorders.Curr HIV Res. 2014;12(2):85-96. doi: 10.2174/1570162x12666140526114526. Curr HIV Res. 2014. PMID: 24862333 Free PMC article. Review.
Cited by
-
The Phenotype of Monocytes in Anterior Uveitis Depends on the HLA-B27 Status.Front Immunol. 2018 Jul 30;9:1773. doi: 10.3389/fimmu.2018.01773. eCollection 2018. Front Immunol. 2018. PMID: 30105034 Free PMC article.
-
Increased viability but decreased culturability of Mycobacterium avium subsp. paratuberculosis in macrophages from inflammatory bowel disease patients under Infliximab treatment.Med Microbiol Immunol. 2015 Dec;204(6):647-56. doi: 10.1007/s00430-015-0393-2. Epub 2015 Feb 22. Med Microbiol Immunol. 2015. PMID: 25702170
-
Anti-TNF-α Drugs Differently Affect the TNFα-sTNFR System and Monocyte Subsets in Patients with Psoriasis.PLoS One. 2016 Dec 9;11(12):e0167757. doi: 10.1371/journal.pone.0167757. eCollection 2016. PLoS One. 2016. PMID: 27936119 Free PMC article.
-
Insensitivity versus poor response to tumour necrosis factor inhibitors in rheumatoid arthritis: a retrospective cohort study.Arthritis Res Ther. 2020 Mar 4;22(1):41. doi: 10.1186/s13075-020-2122-5. Arthritis Res Ther. 2020. PMID: 32131890 Free PMC article.
-
Down-regulation of common NFκB-iNOS pathway by chronic Thalidomide treatment improves Hepatopulmonary Syndrome and Muscle Wasting in rats with Biliary Cirrhosis.Sci Rep. 2016 Dec 23;6:39405. doi: 10.1038/srep39405. Sci Rep. 2016. PMID: 28009008 Free PMC article.
References
-
- Sartor RB. Mechanisms of disease: pathogenesis of Crohn's disease and ulcerative colitis. Nat Clin Pract Gastroenterol Hepatol. 2006;3:390–407. - PubMed
-
- Magro F, Portela F. Management of inflammatory bowel disease with infliximab and other anti-tumor necrosis factor alpha therapies. BioDrugs. 2010;24(Suppl. 1):3–14. - PubMed
-
- Osterman MT, Lichtenstein GR. Current and future anti-TNF therapy for inflammatory bowel disease. Curr Treat Options Gastroenterol. 2007;10:195–207. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
