

Can Italian healthcare administrative databases be used to compare regions with respect to compliance with standards of care for chronic diseases?
- PMID: 24816637
- PMCID: PMC4015953
- DOI: 10.1371/journal.pone.0095419
Can Italian healthcare administrative databases be used to compare regions with respect to compliance with standards of care for chronic diseases?
Abstract
Background: Italy has a population of 60 million and a universal coverage single-payer healthcare system, which mandates collection of healthcare administrative data in a uniform fashion throughout the country. On the other hand, organization of the health system takes place at the regional level, and local initiatives generate natural experiments. This is happening in particular in primary care, due to the need to face the growing burden of chronic diseases. Health services research can compare and evaluate local initiatives on the basis of the common healthcare administrative data.However reliability of such data in this context needs to be assessed, especially when comparing different regions of the country. In this paper we investigated the validity of healthcare administrative databases to compute indicators of compliance with standards of care for diabetes, ischaemic heart disease (IHD) and heart failure (HF).
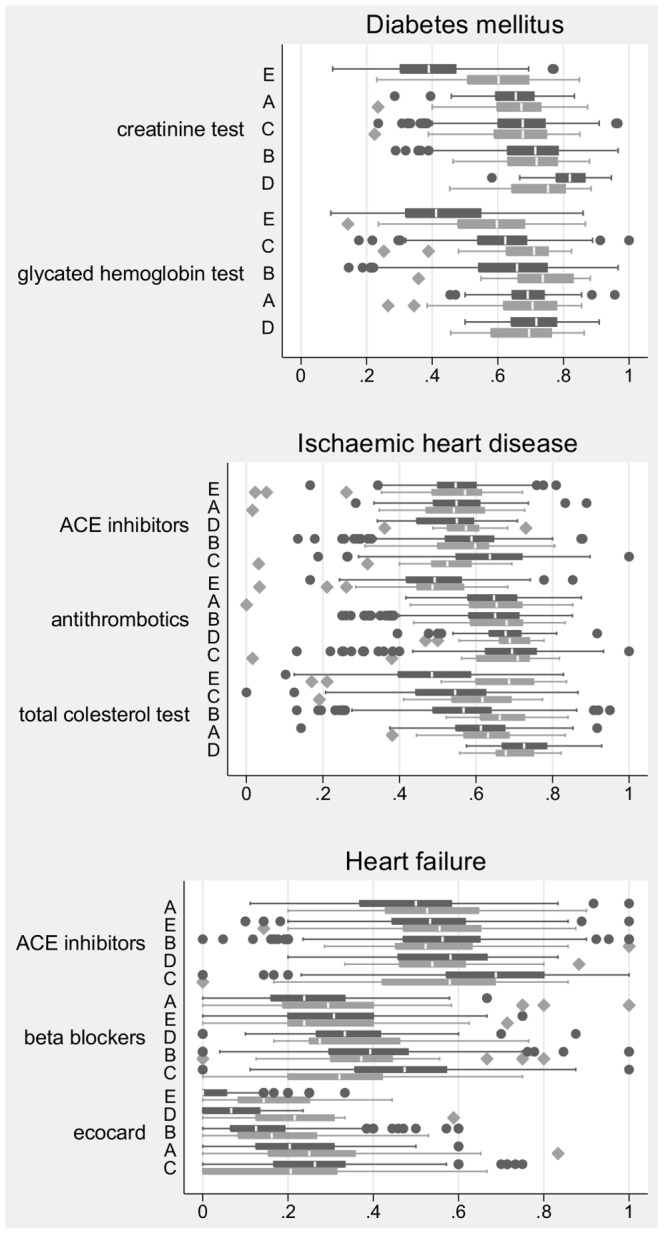
Methods: We compared indicators estimated from healthcare administrative data collected by Local Health Authorities in five Italian regions with corresponding estimates from clinical data collected by General Practitioners (GPs). Four indicators of diagnostic follow-up (two for diabetes, one for IHD and one for HF) and four indicators of appropriate therapy (two each for IHD and HF) were considered.
Results: Agreement between the two data sources was very good, except for indicators of laboratory diagnostic follow-up in one region and for the indicator of bioimaging diagnostic follow-up in all regions, where measurement with administrative data underestimated quality.
Conclusion: According to evidence presented in this study, estimating compliance with standards of care for diabetes, ischaemic heart disease and heart failure from healthcare databases is likely to produce reliable results, even though completeness of data on diagnostic procedures should be assessed first. Performing studies comparing regions using such indicators as outcomes is a promising development with potential to improve quality governance in the Italian healthcare system.
Conflict of interest statement
Figures
References
-
- Starfield B (2010) Reinventing primary care: lessons from canada for the united states. Health affairs (Project Hope) 29: 1030–1036. - PubMed
-
- Barnes KA, Kroening-Roche JC, Comfort BW (2012) The developing vision of primary care. New England Journal of Medicine 367: 891–893. - PubMed
-
- Ettelt S, Mays N (2011) Health services research in europe and its use for informing policy. Journal of Health Services Research & Policy 16: 48–60. - PubMed
-
- Klazinga N, Fischer C, ten Asbroek A (2011) Health services research related to performance indicators and benchmarking in europe. Journal of Health Services Research & Policy 16: 38–47. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
