

Prevalence of dyslipidemia in urban and rural India: the ICMR-INDIAB study
- PMID: 24817067
- PMCID: PMC4016101
- DOI: 10.1371/journal.pone.0096808
Prevalence of dyslipidemia in urban and rural India: the ICMR-INDIAB study
Abstract
Aim: To study the pattern and prevalence of dyslipidemia in a large representative sample of four selected regions in India.
Methods: Phase I of the Indian Council of Medical Research-India Diabetes (ICMR-INDIAB) study was conducted in a representative population of three states of India [Tamil Nadu, Maharashtra and Jharkhand] and one Union Territory [Chandigarh], and covered a population of 213 million people using stratified multistage sampling design to recruit individuals ≥20 years of age. All the study subjects (n = 16,607) underwent anthropometric measurements and oral glucose tolerance tests were done using capillary blood (except in self-reported diabetes). In addition, in every 5th subject (n = 2042), a fasting venous sample was collected and assayed for lipids. Dyslipidemia was diagnosed using National Cholesterol Education Programme (NCEP) guidelines.
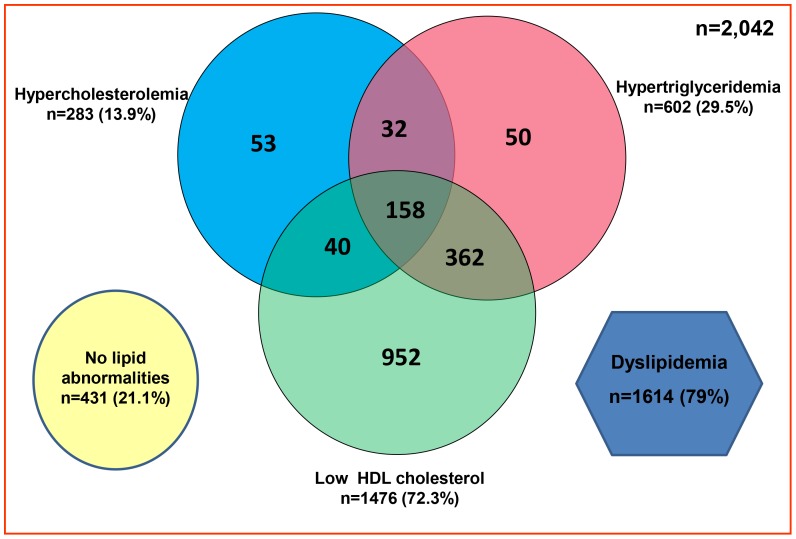
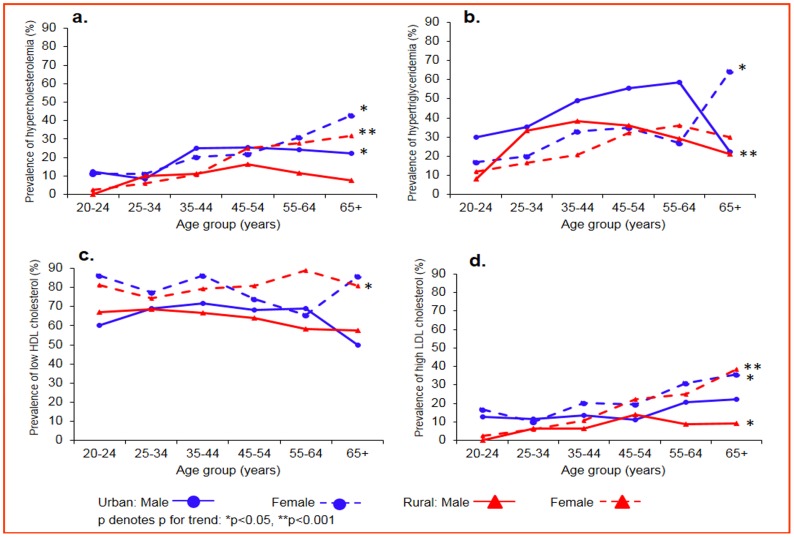
Results: Of the subjects studied, 13.9% had hypercholesterolemia, 29.5% had hypertriglyceridemia, 72.3% had low HDL-C, 11.8% had high LDL-C levels and 79% had abnormalities in one of the lipid parameters. Regional disparity exists with the highest rates of hypercholesterolemia observed in Tamilnadu (18.3%), highest rates of hypertriglyceridemia in Chandigarh (38.6%), highest rates of low HDL-C in Jharkhand (76.8%) and highest rates of high LDL-C in Tamilnadu (15.8%). Except for low HDL-C and in the state of Maharashtra, in all other states, urban residents had the highest prevalence of lipid abnormalities compared to rural residents. Low HDL-C was the most common lipid abnormality (72.3%) in all the four regions studied; in 44.9% of subjects, it was present as an isolated abnormality. Common significant risk factors for dyslipidemia included obesity, diabetes, and dysglycemia.
Conclusion: The prevalence of dyslipidemia is very high in India, which calls for urgent lifestyle intervention strategies to prevent and manage this important cardiovascular risk factor.
Conflict of interest statement
Figures
References
-
- Mathers C, Fat DM, Boerma JT (2008) for World Health Organization. The Global Burden of Disease: 2004 Update. Geneva: World Health Organization.
-
- Fuster V, Kelly BB, editors (2010) Promoting Cardiovascular Health in the Developing World: A Critical Challenge to Achieve Global Health. Washginton, DC: National Academies Press. - PubMed
-
- Sample Registration System (2007) Million Death Study: Preliminary Report on Causes of Death in India 2001–2003. New Delhi: Registrar General of India.
-
- Enas EA, Yusuf S, Mehta J (1992) Prevalence of coronary artery disease in Asian Indians. Am J Cardiol 70: 945–949. - PubMed
-
- Omran AR (1971) The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem Fund Q 49: 509–538. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
