

Subsequent Adenomas of Ileal Pouch and Anorectal Segment after Prophylactic Surgery for Familial Adenomatous Polyposis
- PMID: 24817992
- PMCID: PMC4012278
Subsequent Adenomas of Ileal Pouch and Anorectal Segment after Prophylactic Surgery for Familial Adenomatous Polyposis
Abstract
Familial adenomatous polyposis (FAP) is an autosomally dominant disease characterized by the early development of colorectal adenomas and carcinoma in untreated patients. Patients with FAP may develop rectal cancer at their initial presentation (primary) or after prophylactic surgery (secondary). Controversies exist regarding which surgical procedure represents the best first-line treatment. The options for FAP are ileorectal anastomosis (IRA) or a restorative proctocolectomy (RPC) with either a handsewn or a stapled ileal pouch-anal anastomosis (IPAA), with or without mucosectomy. The purpose of these surgeries is to stop progression to an adenoma-cancer sequence by eradicating the colon, a disease prone organ. Unfortunately, these surgical procedures, which excise the entire colon and rectum while maintaining transanal fecal continence, do not guarantee that patients still won't develop adenomas. Based on the available literature, we therefore reviewed reported incidences of pouch-related adenomas that occurred post prophylactic surgery for FAP. The review consists of a collection of case, descriptive, prospective and retrospective reports.
Objectives: To provide available data on the natural history of subsequent adenomas after prophylactic surgery (by type) for FAP.
Methods: A review was conducted of existing case, descriptive, prospective and retrospective reports for patients undergoing prophylactic surgery for FAP (1975 - August, 2013). In each case, the adenomas were clearly diagnosed in one of the following: the ileal pouch mucosa (above the ileorectal anastomosis), within the anorectal segment (ARS) below the ileorectal anastomosis, or in the afferent ileal loop.
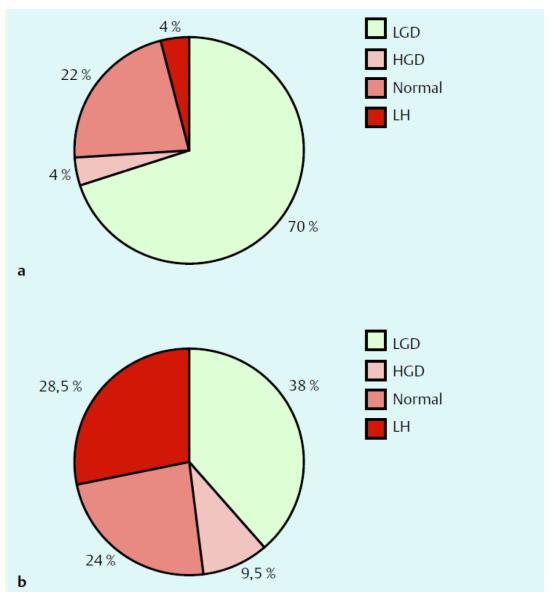
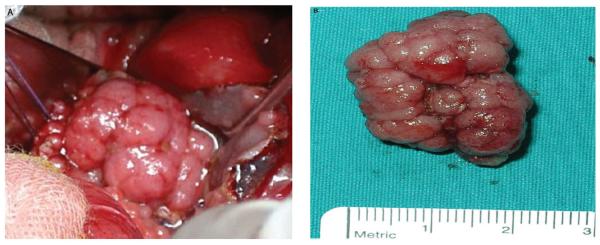
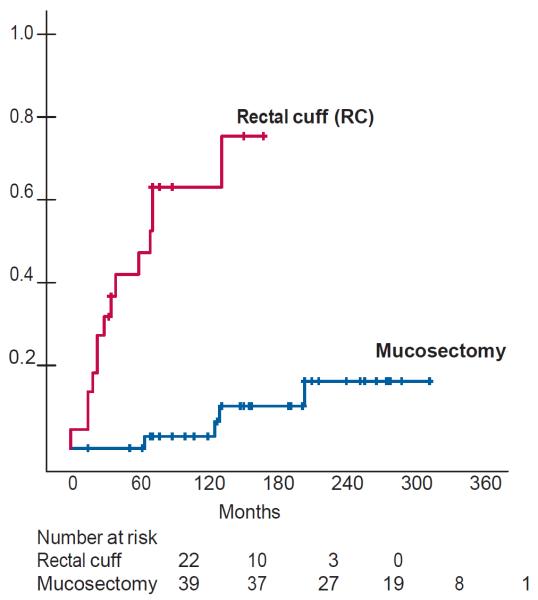
Results: A total of 515 (36%) patients with pouch-related adenomas have been reported. Two hundred and eleven (211) patients had adenomas in the ileal pouch mucosa, 295 had them in the ARS and in 9 were in the afferent ileal loop. Patients with pouch adenomas without dysplasia or cancer were either endoscopically polypectomized or were treated with a coagulation modality using either a Nd:Yag laser or argon plasma coagulation (as indicated). Patients with dysplastic pouch adenomas or pouch adenomas with cancer had their pouch excised (pouchectomy).
Conclusion: In patients with FAP treated with IRA or RPC with IPAA, the formation of adenomas in the pouch-body mucosa or ARS/anastomosis and in the afferent ileal loop is apparent. Because of risks for adenoma recurrence, a life time endoscopic pouch-surveillance is warranted.
Keywords: Familial-adenomatous polyposis; adenomas; ileal-anal pouch anastomosis; ileorectal anastomosis; restorative proctocolectomy.
Figures
Similar articles
-
Endoscopic management of patients with familial adenomatous polyposis after prophylactic colectomy or restorative proctocolectomy - systematic review of the literature.Radiol Oncol. 2024 Jun 11;58(2):153-169. doi: 10.2478/raon-2024-0029. eCollection 2024 Jun 1. Radiol Oncol. 2024. PMID: 38860690 Free PMC article.
-
Adenocarcinomas After Prophylactic Surgery For Familial Adenomatous Polyposis.J Cancer Ther. 2013;4(1):260-270. doi: 10.4236/jct.2013.41033. J Cancer Ther. 2013. PMID: 23875116 Free PMC article.
-
Prevalence and risk factors for adenomas in the ileal pouch and the afferent loop after restorative proctocolectomy for patients with familial adenomatous polyposis.Surg Endosc. 2013 Oct;27(10):3816-22. doi: 10.1007/s00464-013-2980-x. Epub 2013 May 1. Surg Endosc. 2013. PMID: 23636532
-
Cancer in an unexpected site post pouch surgery for familial adenomatous polyposis (FAP).Int J Surg Case Rep. 2018;42:266-268. doi: 10.1016/j.ijscr.2017.12.037. Epub 2017 Dec 28. Int J Surg Case Rep. 2018. PMID: 29324375 Free PMC article.
-
Restorative proctocolectomy and ileal pouch-anal anastomosis for familial adenomatous polyposis revisited.Fam Cancer. 2006;5(3):241-60; discussion 261-2. doi: 10.1007/s10689-005-5672-4. Fam Cancer. 2006. PMID: 16998670 Review.
Cited by
-
Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management.Am J Gastroenterol. 2017 Oct;112(10):1509-1525. doi: 10.1038/ajg.2017.212. Epub 2017 Aug 8. Am J Gastroenterol. 2017. PMID: 28786406 Review.
-
Segmental resection with primary anastomosis is not always safe in splenic flexure perforation.BMC Res Notes. 2016 Jan 16;9:27. doi: 10.1186/s13104-016-1841-9. BMC Res Notes. 2016. PMID: 26774506 Free PMC article.
-
Updated European guidelines for clinical management of familial adenomatous polyposis (FAP), MUTYH-associated polyposis (MAP), gastric adenocarcinoma, proximal polyposis of the stomach (GAPPS) and other rare adenomatous polyposis syndromes: a joint EHTG-ESCP revision.Br J Surg. 2024 May 3;111(5):znae070. doi: 10.1093/bjs/znae070. Br J Surg. 2024. PMID: 38722804 Free PMC article.
References
-
- Kinzler KW, Nilbert MC, Su LK, et al. Identification of FAP locus genes from chromosome 5q21. Science. 1991;253:661–5. - PubMed
-
- Church J. Ileoanal pouch neoplasia in familial adenomatous polyposis: an underestimated threat. Dis Colon Rectum. 2005;48:1708–13. - PubMed
-
- Groden J, Thliveris A, Samowitz W, et al. Identification and characterization of the familial adenomatous polyposis coli gene. Cell. 1991;66:589–600. - PubMed
-
- Linehan G, Cahill RA, Kalimuthu SN, O'Connell F, Redmond HP, Kirwan WO. Adenocarcinoma arising in the ileoanal pouch after restorative proctocolectomy for familial adenomatous polyposis. Int J Colorectal Dis. 2008;23:329–30. - PubMed
-
- Nieuwenhuis MH, De Vos Tot Nederveen Cappel W, Botma A, et al. Desmoid tumors in a dutch cohort of patients with familial adenomatous polyposis. Clin Gastroenterol Hepatol. 2008;6:215–9. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous