

Impact of clipping versus coiling on postoperative hemodynamics and pulmonary edema after subarachnoid hemorrhage
- PMID: 24818154
- PMCID: PMC4000965
- DOI: 10.1155/2014/807064
Impact of clipping versus coiling on postoperative hemodynamics and pulmonary edema after subarachnoid hemorrhage
Abstract
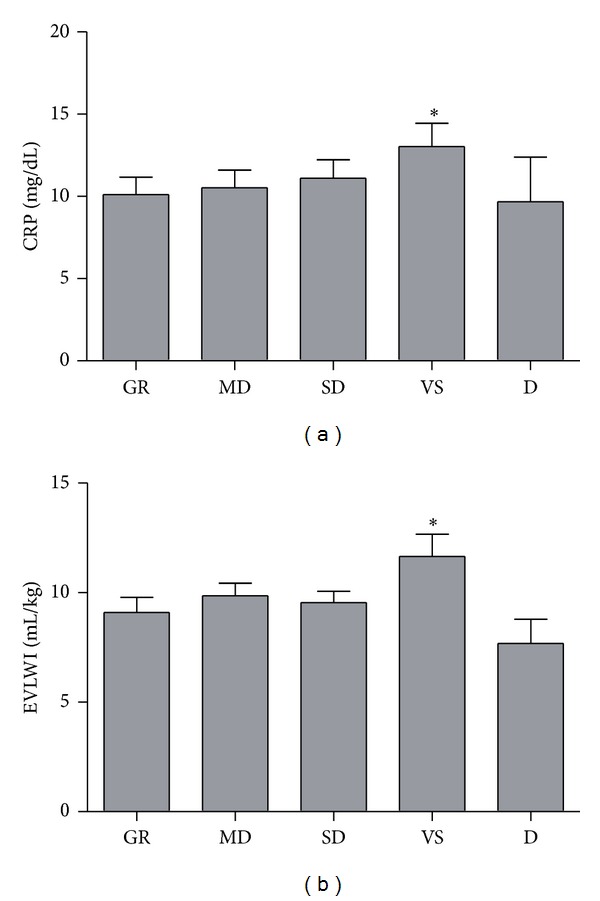
Volume management is critical for assessment of cerebral vasospasm after aneurysmal subarachnoid hemorrhage (SAH). This multicenter prospective cohort study compared the impact of surgical clipping versus endovascular coiling on postoperative hemodynamics and pulmonary edema in patients with SAH. Hemodynamic parameters were measured for 14 days using a transpulmonary thermodilution system. The study included 202 patients, including 160 who underwent clipping and 42 who underwent coiling. There were no differences in global ejection fraction (GEF), cardiac index, systemic vascular resistance index, or global end-diastolic volume index between the clipping and coiling groups in the early period. However, extravascular lung water index (EVLWI) and pulmonary vascular permeability index (PVPI) were significantly higher in the clipping group in the vasospasm period. Postoperative C-reactive protein (CRP) level was higher in the clipping group and was significantly correlated with postoperative brain natriuretic peptide level. Multivariate analysis found that PVPI and GEF were independently associated with high EVLWI in the early period, suggesting cardiogenic edema, and that CRP and PVPI, but not GEF, were independently associated with high EVLWI in the vasospasm period, suggesting noncardiogenic edema. In conclusion, clipping affects postoperative CRP level and may thereby increase noncardiogenic pulmonary edema in the vasospasm period. His trial is registered with University Hospital Medical Information Network UMIN000003794.
Figures



Similar articles
-
A multicenter prospective cohort study of volume management after subarachnoid hemorrhage: circulatory characteristics of pulmonary edema after subarachnoid hemorrhage.J Neurosurg. 2016 Aug;125(2):254-63. doi: 10.3171/2015.6.JNS1519. Epub 2015 Nov 27. J Neurosurg. 2016. PMID: 26613172
-
Comparison of postoperative volume status and hemodynamics between surgical clipping and endovascular coiling in patients after subarachnoid hemorrhage.J Neurosurg Anesthesiol. 2015 Jan;27(1):7-15. doi: 10.1097/ANA.0000000000000066. J Neurosurg Anesthesiol. 2015. PMID: 24733051
-
Optimal range of global end-diastolic volume for fluid management after aneurysmal subarachnoid hemorrhage: a multicenter prospective cohort study.Crit Care Med. 2014 Jun;42(6):1348-56. doi: 10.1097/CCM.0000000000000163. Crit Care Med. 2014. PMID: 24394632
-
Transpulmonary Thermodilution: Its Role in Assessment of Lung Water and Pulmonary Edema.J Cardiothorac Vasc Anesth. 2017 Aug;31(4):1471-1480. doi: 10.1053/j.jvca.2017.02.018. Epub 2017 Feb 4. J Cardiothorac Vasc Anesth. 2017. PMID: 28465120 Review.
-
Transpulmonary Thermodilution-Based Management of Neurogenic Pulmonary Edema After Subarachnoid Hemorrhage.Am J Med Sci. 2015 Nov;350(5):415-9. doi: 10.1097/MAJ.0000000000000561. Am J Med Sci. 2015. PMID: 26517502 Review.
Cited by
-
Risk of fatal sinus arrest induced by low-grade subarachnoid hemorrhage: A case of a young patient with obstructive sleep apnea.Surg Neurol Int. 2020 Jun 20;11:156. doi: 10.25259/SNI_66_2020. eCollection 2020. Surg Neurol Int. 2020. PMID: 32637209 Free PMC article.
References
-
- Bederson JB, Connolly ES, Jr., Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the stroke council, American heart association. Stroke. 2009;40(3):994–1025. - PubMed
-
- Treggiar MM. Hemodynamic management of subarachnoid hemorrhage. Neurocritical Care. 2011;15(2):329–335. - PubMed
-
- Wolf S. Routine management of volume status after aneurysmal subarachnoid hemorrhage. Neurocritical Care. 2011;15(2):275–280. - PubMed
-
- Lazaridis C. Advanced hemodynamic monitoring: principles and practice in neurocritical care. Neurocritical Care. 2012;16(1):163–169. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
