

Complication rates of ostomy surgery are high and vary significantly between hospitals
- PMID: 24819104
- PMCID: PMC4197143
- DOI: 10.1097/DCR.0000000000000038
Complication rates of ostomy surgery are high and vary significantly between hospitals
Abstract
Background: Ostomy surgery is common and has traditionally been associated with high rates of morbidity and mortality, suggesting an important target for quality improvement.
Objective: The purpose of this work was to evaluate the variation in outcomes after ostomy creation surgery within Michigan to identify targets for quality improvement.
Design: This was a retrospective cohort study.
Settings: The study took place within the 34-hospital Michigan Surgical Quality Collaborative.
Patients: Patients included were those undergoing ostomy creation surgery between 2006 and 2011.
Main outcome measures: We evaluated hospital morbidity and mortality rates after risk adjustment (age, comorbidities, emergency vs elective, and procedure type).
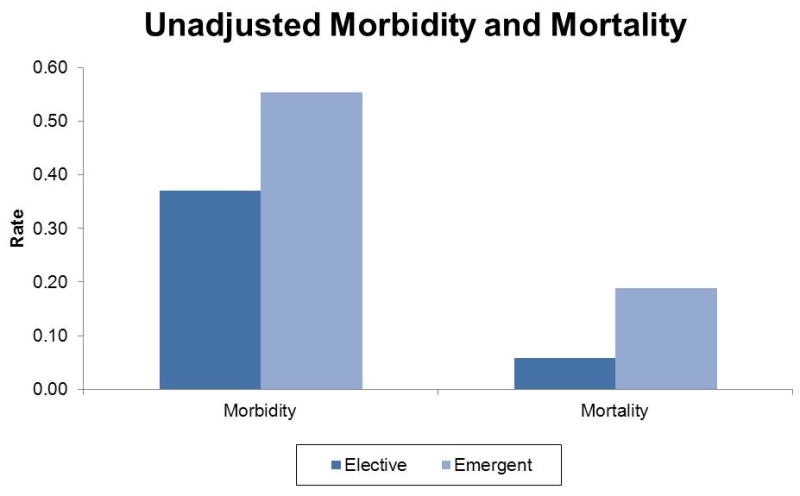
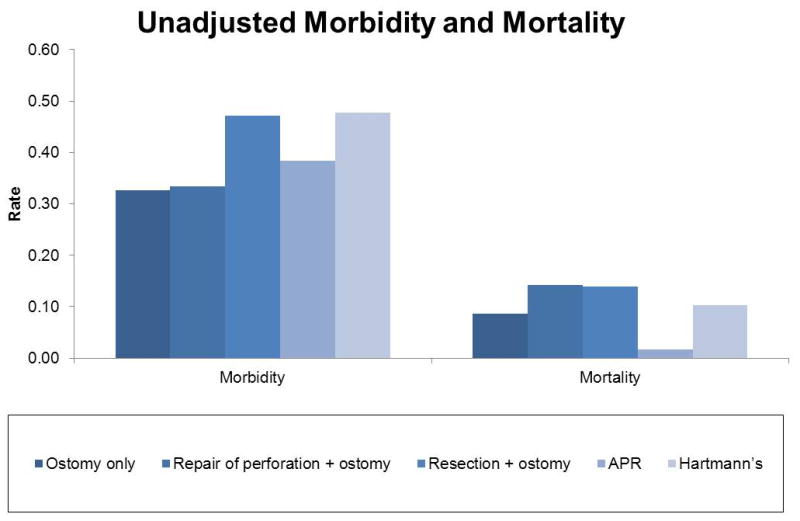
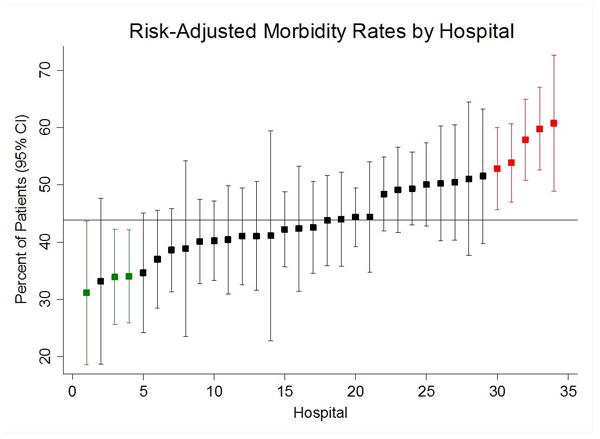
Results: A total of 4250 patients underwent ostomy creation surgery; 3866 procedures (91.0%) were open and 384 (9.0%) were laparoscopic. Unadjusted morbidity and mortality rates were 43.9% and 10.7%. Unadjusted morbidity rates for specific procedures ranged from 32.7% for ostomy-creation-only procedures to 47.8% for Hartmann procedures. Risk-adjusted morbidity rates varied significantly between hospitals, ranging from 31.2% (95% CI, 18.4-43.9) to 60.8% (95% CI, 48.9-72.6). There were 5 statistically significant high-outlier hospitals and 3 statistically significant low-outlier hospitals for risk-adjusted morbidity. The pattern of complication types was similar between high- and low-outlier hospitals. Case volume, operative duration, and use of laparoscopic surgery did not explain the variation in morbidity rates across hospitals.
Limitations: This work was limited by its retrospective study design, by unmeasured variation in case severity, and by our inability to differentiate between colostomies and ileostomies because of the use of Current Procedural Terminology codes.
Conclusions: Morbidity and mortality rates for modern ostomy surgery are high. Although this type of surgery has received little attention in healthcare policy, these data reveal that it is both common and uncommonly morbid. Variation in hospital performance provides an opportunity to identify quality improvement practices that could be disseminated among hospitals.
Conflict of interest statement
Figures

Similar articles
-
Outcome and Timing of Ostomy Reversal Surgery for Diverticular Disease in Veterans Administration Hospitals.Am Surg. 2023 Apr;89(4):656-664. doi: 10.1177/00031348211034764. Epub 2021 Aug 4. Am Surg. 2023. PMID: 34346712
-
The importance of improving the quality of emergency surgery for a regional quality collaborative.Ann Surg. 2013 Apr;257(4):596-602. doi: 10.1097/SLA.0b013e3182863750. Ann Surg. 2013. PMID: 23470507 Free PMC article.
-
Hospital complication rates with bariatric surgery in Michigan.JAMA. 2010 Jul 28;304(4):435-42. doi: 10.1001/jama.2010.1034. JAMA. 2010. PMID: 20664044
-
Patients' perspectives of care and surgical outcomes in Michigan: an analysis using the CAHPS hospital survey.Ann Surg. 2014 Jul;260(1):5-9. doi: 10.1097/SLA.0000000000000626. Ann Surg. 2014. PMID: 24646549 Free PMC article.
-
Outcomes of ostomy procedures in patients aged 70 years and older.Arch Surg. 2003 Oct;138(10):1077-82. doi: 10.1001/archsurg.138.10.1077. Arch Surg. 2003. PMID: 14557123
Cited by
-
The Impact of Colostomy on Inpatient Outcomes Following Primary Total Knee Arthroplasty.Cureus. 2024 Jul 31;16(7):e65900. doi: 10.7759/cureus.65900. eCollection 2024 Jul. Cureus. 2024. PMID: 39092377 Free PMC article.
-
Marginalization in the Medical Encounter: Ostomy Patients Experience of Perceived Stigmatizing Sentiments from Medical Clinicians.SAGE Open Nurs. 2022 Apr 24;8:23779608221095315. doi: 10.1177/23779608221095315. eCollection 2022 Jan-Dec. SAGE Open Nurs. 2022. PMID: 35493541 Free PMC article.
-
The rate of ileostomy site incisional hernias: more common than we think?Hernia. 2024 Dec;28(6):2311-2320. doi: 10.1007/s10029-024-03163-0. Epub 2024 Sep 26. Hernia. 2024. PMID: 39325325 Free PMC article.
-
Ostomy continence devices: a systematic review of the literature and meta-analysis.Colorectal Dis. 2024 Apr;26(4):622-631. doi: 10.1111/codi.16906. Epub 2024 Feb 15. Colorectal Dis. 2024. PMID: 38358053 Free PMC article.
-
Comparison of Outcomes Between Total Abdominal and Partial Colectomy for the Management of Severe, Complicated Clostridium Difficile Infection.J Am Coll Surg. 2019 Jun;228(6):925-930. doi: 10.1016/j.jamcollsurg.2018.11.015. Epub 2018 Dec 18. J Am Coll Surg. 2019. PMID: 30576799 Free PMC article.
References
-
- Goldberg M, Aukett LK, Carmel J, et al. Management of the patient with a fecal ostomy: best practice guideline for clinicians. J Wound Ostomy Continence Nurs. 2010;37:596–598. - PubMed
-
- Sandler RS, Everhart JE, Donowitz M, et al. The burden of selected digestive diseases in the United States. Gastroenterology. 2002;122:1500–1511. - PubMed
-
- U S Cancer Statistics Working Group-United States Cancer Statistics: 1999-2009 Incidence and Mortality Data. Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute; 2012. Volume Available at http://www.cdc.gov/uscs.
-
- Robertson I, Leung E, Hughes D, et al. Prospective analysis of stoma-related complications. Colorectal Dis. 2005;7:279–285. - PubMed
-
- Duron JJ, Duron E, Dugue T, et al. Risk factors for mortality in major digestive surgery in the elderly: a multicenter prospective study. Ann Surg. 2011;254:375–382. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
