

The use of ultrasound in the search for the primary site of unknown primary head and neck squamous cell cancers
- PMID: 24819862
- PMCID: PMC4696034
- DOI: 10.1016/j.oraloncology.2014.03.015
The use of ultrasound in the search for the primary site of unknown primary head and neck squamous cell cancers
Abstract
Background: Although human papillomavirus detection in cervical lymph nodes of head and neck squamous cell cancers (HNSCC) of unknown primary site (UP) is indicative of a primary tumor of the oropharynx (OP), localization can remain elusive. Therefore, we investigated ultrasonography (US) for the identification of the primary tumor.
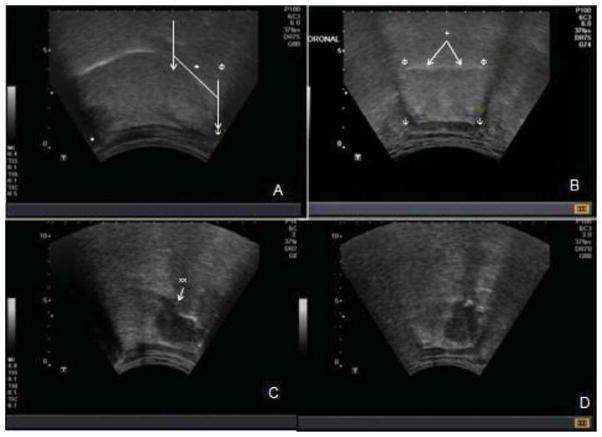
Methods: Eligible cases had HNSCC of UP after evaluation by a head and neck surgical oncologist. Controls were healthy volunteers. Transcervical and intraoral ultrasonography was performed by a standard protocol using convex (3.75-6.0 MHz and 5-7.5 MHz) transducers. US findings were compared with operative examination (exam under anesthesia, direct laryngoscopy) and biopsies. The primary outcome of interest was the presence or absence of a lesion on US.
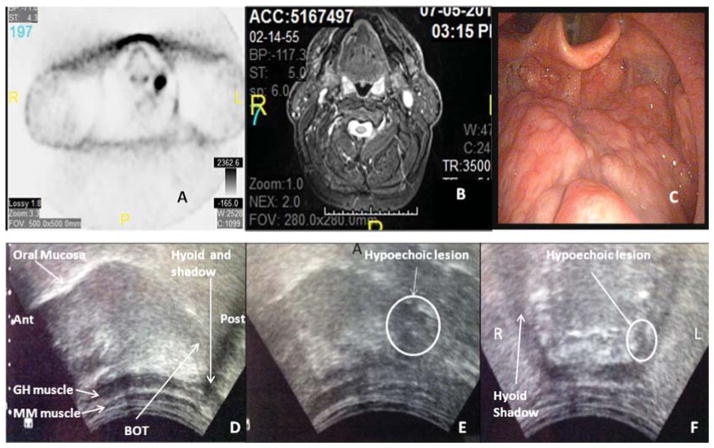
Results: 10 cases and 20 controls were enrolled. PET/CT scans were negative/nonspecific (9), or suspicious (1) for a primary lesion. On US, predominantly hypoechoic (9 of 10) lesions were visualized consistent with base of tongue (n=7) or tonsil (n=3) primary tumors. On operative examination, 5 of 10 were appreciated. Two additional primaries were confirmed with biopsies "directed" by preoperative US. This represents an overall diagnostic rate of 70%, which is 20% higher than our detection rate for 2008-2010. The three cases in which a suspicious lesion was visualized on US, yet remained UP despite further interventions, could represent false positives, misclassification or operator variability. No lesions were suspected among the controls.
Conclusion: Ultrasound has promise for detection of UPs of the OP and therefore warrants further investigation.
Keywords: Head and neck cancer; Human papillomavirus (HPV); Oropharynx neoplasm; Ultrasonography; Unknown primary.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Surgeon-performed intraoperative transoral ultrasound improves the detection of human papillomavirus-positive head and neck cancers of unknown primary.Oral Oncol. 2024 Dec;159:107073. doi: 10.1016/j.oraloncology.2024.107073. Epub 2024 Oct 14. Oral Oncol. 2024. PMID: 39406014
-
18 F-FDG PET/CT vs. human papillomavirus, p16 and Epstein-Barr virus detection in cervical metastatic lymph nodes for identifying primary tumors.Int J Cancer. 2017 Mar 15;140(6):1405-1412. doi: 10.1002/ijc.30550. Int J Cancer. 2017. PMID: 27943271
-
Transcervical ultrasound identifies primary tumor site of unknown primary head and neck squamous cell carcinoma.Otolaryngol Head Neck Surg. 2014 Dec;151(6):1090-2. doi: 10.1177/0194599814549181. Epub 2014 Sep 5. Otolaryngol Head Neck Surg. 2014. PMID: 25193515 Free PMC article. No abstract available.
-
Cervical lymph node metastases of squamous cell carcinoma from an unknown primary.Cancer Treat Rev. 2004 Apr;30(2):153-64. doi: 10.1016/j.ctrv.2003.10.001. Cancer Treat Rev. 2004. PMID: 15023433 Review.
-
Unknown primary detected by FDG-PET. A review of the present indications of FDG-PET in head and neck cancers.Acta Otorhinolaryngol Belg. 2002;56(1):77-82. Acta Otorhinolaryngol Belg. 2002. PMID: 11894635 Review.
Cited by
-
Concordance of oral HPV prevalence between patients with oropharyngeal cancer and their partners.Infect Agent Cancer. 2016 Apr 27;11:21. doi: 10.1186/s13027-016-0066-9. eCollection 2016. Infect Agent Cancer. 2016. PMID: 27123042 Free PMC article.
-
Trends in Risks for Second Primary Cancers Associated With Index Human Papillomavirus-Associated Cancers.JAMA Netw Open. 2018 Sep 7;1(5):e181999. doi: 10.1001/jamanetworkopen.2018.1999. JAMA Netw Open. 2018. PMID: 30646145 Free PMC article.
-
Feasibility of Use of the 8th Edition of the American Joint Committee on Cancer Staging for Head and Neck Cancers in Indian Scenario: An Evaluative Study.Ann Maxillofac Surg. 2021 Jan-Jun;11(1):27-31. doi: 10.4103/ams.ams_125_20. Epub 2021 Jul 24. Ann Maxillofac Surg. 2021. PMID: 34522650 Free PMC article.
-
Epidemiology of Human Papillomavirus-Positive Head and Neck Squamous Cell Carcinoma.J Clin Oncol. 2015 Oct 10;33(29):3235-42. doi: 10.1200/JCO.2015.61.6995. Epub 2015 Sep 8. J Clin Oncol. 2015. PMID: 26351338 Free PMC article. Review.
-
On the reproducibility of expert-operated and robotic ultrasound acquisitions.Int J Comput Assist Radiol Surg. 2017 Jun;12(6):1003-1011. doi: 10.1007/s11548-017-1561-1. Epub 2017 Mar 20. Int J Comput Assist Radiol Surg. 2017. PMID: 28321804
References
-
- Strojan P, Ferlito A, Medina JE, Woolgar JA, Rinaldo A, Robbins KT, et al. Contemporary management of lymph node metastases from an unknown primary to the neck: I. A review of diagnostic approaches. Head Neck. 2013;35:123–32. - PubMed
-
- Vent J, Haidle B, Wedemeyer I, Huebbers C, Siefer O, Semrau R, et al. p16 Expression in carcinoma of unknown primary: diagnostic indicator and prognostic marker. Head Neck. 2013 - PubMed
-
- Gillison ML, D’Souza G, Westra W, Sugar E, Xiao W, Begum S, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst. 2008;100:407–20. - PubMed
-
- Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008;100:261–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
