

Impact of ART on TB case fatality stratified by CD4 count for HIV-positive TB patients in Cape Town, South Africa (2009-2011)
- PMID: 24820105
- PMCID: PMC4161924
- DOI: 10.1097/QAI.0000000000000201
Impact of ART on TB case fatality stratified by CD4 count for HIV-positive TB patients in Cape Town, South Africa (2009-2011)
Abstract
Objective: To identify determinants of tuberculosis (TB) case fatality including the impact of antiretroviral therapy (ART) at different CD4 thresholds for HIV-positive adult and adolescent TB patients.
Methods: Through a retrospective analysis of the electronic TB database, we identified the HIV status of newly registered patients aged ≥15 years. Multivariable Cox proportional hazard models were used to determine the risk factors for TB case fatality in these patients.
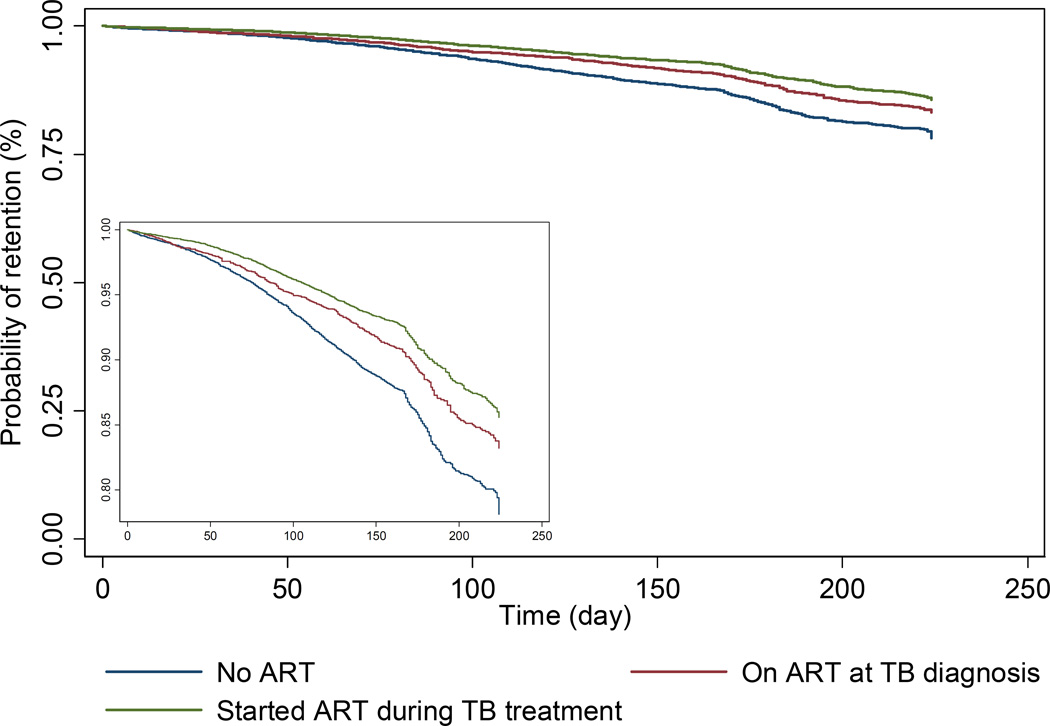
Results: In 2009, 2010, and 2011, 25,841, 26,104, and 25,554 newly registered adult TB patients were treated in primary health care clinics in Cape Town, of whom 49.7%, 50.4%, and 50.9% were HIV positive. ART uptake increased over 3 years from 43% to 64.9%, and case fatality of the HIV-positive patients decreased from 7.0% to 5.8% (P < 0.001). Female gender, increasing age, retreatment TB, low CD4 counts, and extrapulmonary TB were associated with increased case fatality, whereas patients on ART had a substantial decrease in case fatality. The difference in case fatality between patients on ART and not on ART was most pronounced at low CD4 counts with the positive influence of ART noted up to a CD4 count threshold of 350 cells per cubic millimeter (P < 0.001). Despite improvements in ART uptake, in 2011, 21% of the patients with CD4 counts <350 cells per cubic millimeter did not start ART during TB treatment.
Conclusion: This study showed a relatively poor uptake of ART among severely immune-compromised TB patients. Patients with CD4 counts <350 cells per cubic millimeter were shown to clearly benefit from ART during TB treatment, and ART initiation should be prioritized for this category of patients.
Conflict of interest statement
The authors have no conflicts of interest.
Figures





References
-
- Mukadi YD, Maher D, Harries A. Tuberculosis case fatality rates in high HIV prevalence populations in sub-Saharan Africa. AIDS. 2001;15:143–152. - PubMed
-
- World Health Organisation. Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. 2010 revision. Available at http://whqlibdoc.who.int/publications/2010/9789241599764_eng.pdf. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
