

Preventing 30-day hospital readmissions: a systematic review and meta-analysis of randomized trials
- PMID: 24820131
- PMCID: PMC4249925
- DOI: 10.1001/jamainternmed.2014.1608
Preventing 30-day hospital readmissions: a systematic review and meta-analysis of randomized trials
Abstract
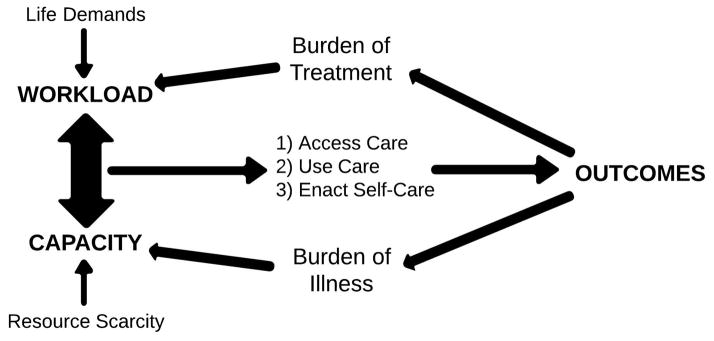
Importance: Reducing early (<30 days) hospital readmissions is a policy priority aimed at improving health care quality. The cumulative complexity model conceptualizes patient context. It predicts that highly supportive discharge interventions will enhance patient capacity to enact burdensome self-care and avoid readmissions.
Objective: To synthesize the evidence of the efficacy of interventions to reduce early hospital readmissions and identify intervention features--including their impact on treatment burden and on patients' capacity to enact postdischarge self-care--that might explain their varying effects.
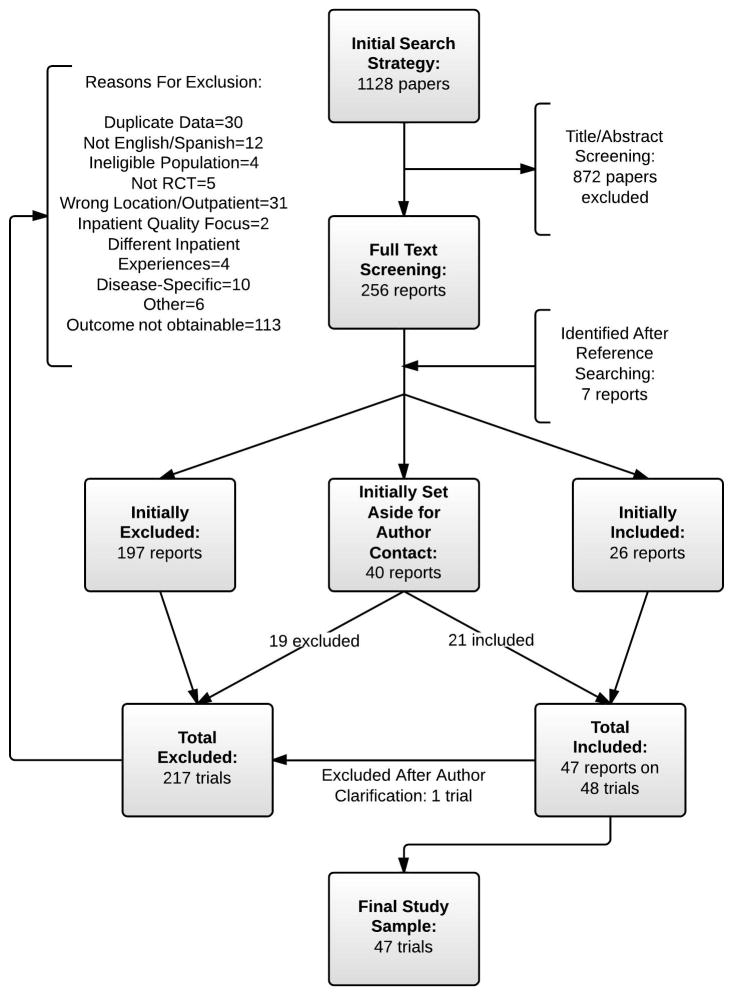
Data sources: We searched PubMed, Ovid MEDLINE, Ovid EMBASE, EBSCO CINAHL, and Scopus (1990 until April 1, 2013), contacted experts, and reviewed bibliographies.
Study selection: Randomized trials that assessed the effect of interventions on all-cause or unplanned readmissions within 30 days of discharge in adult patients hospitalized for a medical or surgical cause for more than 24 hours and discharged to home.
Data extraction and synthesis: Reviewer pairs extracted trial characteristics and used an activity-based coding strategy to characterize the interventions; fidelity was confirmed with authors. Blinded to trial outcomes, reviewers noted the extent to which interventions placed additional work on patients after discharge or supported their capacity for self-care in accordance with the cumulative complexity model.
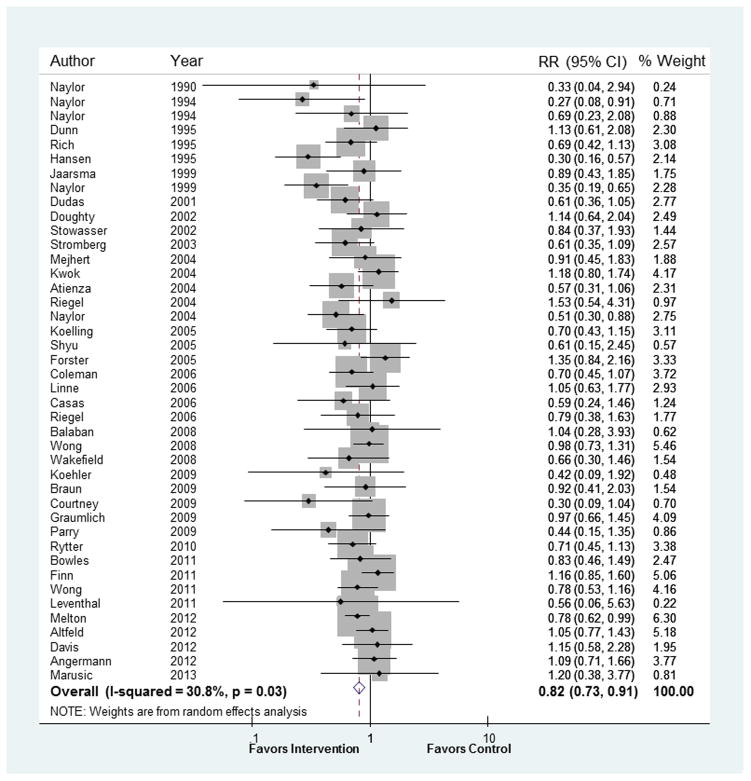
Main outcomes and measures: Relative risk of all-cause or unplanned readmission with or without out-of-hospital deaths at 30 days postdischarge.
Results: In 42 trials, the tested interventions prevented early readmissions (pooled random-effects relative risk, 0.82 [95% CI, 0.73-0.91]; P < .001; I² = 31%), a finding that was consistent across patient subgroups. Trials published before 2002 reported interventions that were 1.6 times more effective than those tested later (interaction P = .01). In exploratory subgroup analyses, interventions with many components (interaction P = .001), involving more individuals in care delivery (interaction P = .05), and supporting patient capacity for self-care (interaction P = .04) were 1.4, 1.3, and 1.3 times more effective than other interventions, respectively. A post hoc regression model showed incremental value in providing comprehensive, postdischarge support to patients and caregivers.
Conclusions and relevance: Tested interventions are effective at reducing readmissions, but more effective interventions are complex and support patient capacity for self-care. Interventions tested more recently are less effective.
Conflict of interest statement
Figures
Comment in
-
Preventing early readmissions.JAMA. 2014 Oct 1;312(13):1344-5. doi: 10.1001/jama.2014.9473. JAMA. 2014. PMID: 25268442 No abstract available.
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009 Apr 2;360(14):1418–1428. - PubMed
-
- Institute of Medicine. Rewarding Provider Performance: Aligning Incentives in Medicare. Washington, DC: 2006.
-
- Medicare Payment Advisory Commission. Report to the Congress: promoting greater efficiency in Medicare. 2007.
-
- Joynt KE, Jha AK. A path forward on Medicare readmissions. N Engl J Med. 2013 Mar 28;368(13):1175–1177. - PubMed
-
- Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumulative complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol. 2012 Oct;65(10):1041–1051. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
