

Adrenal insufficiency in patients with stable non-cystic fibrosis bronchiectasis
- PMID: 24820833
- PMCID: PMC4069733
Adrenal insufficiency in patients with stable non-cystic fibrosis bronchiectasis
Abstract
Background & objectives: Suppressed adrenal responses associated with inhaled steroid use have been reported in patients with bronchiectasis and have been shown to be associated with poor quality of life. This study was undertaken to examine the prevalence of suppressed cortisol responses in stable bronchiectasis and determine their correlation with the use of inhaled corticosteroids, radiologic severity of bronchiectasis and quality of life (QOL) scores.
Methods: In this case-control study, cases were patients with bronchiectasis and suppressed cortisol responses and controls were healthy volunteers, and patients with bronchiectasis without suppressed cortisol responses. Symptoms, lung function test values, exercise capacity, HRCT severity scores for bronchiectasis, exacerbations, inhaled corticosteroid use and quality of life scores were compared between patients with and without suppressed cortisol values.
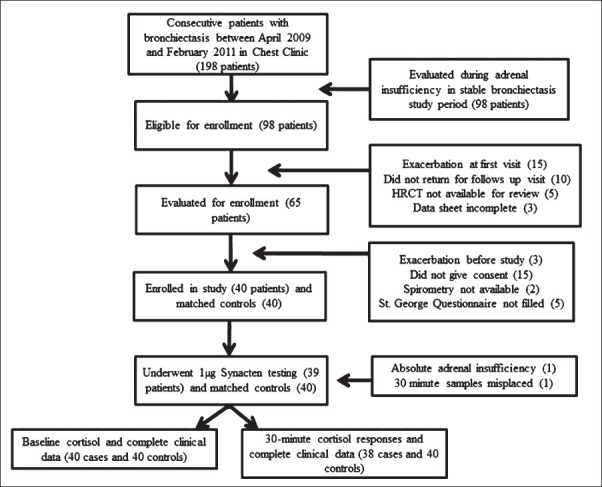
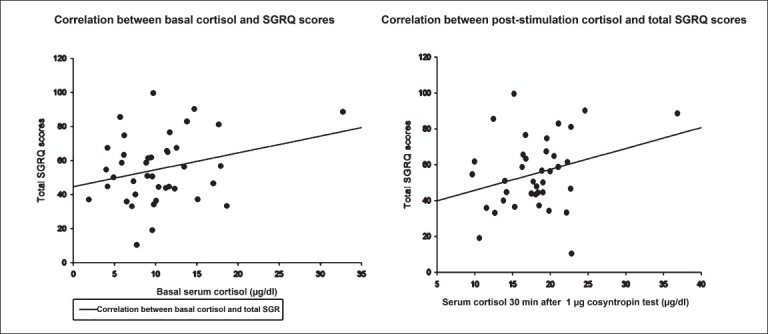
Results: Forty consecutive patients with bronchiectasis and 40 matched controls underwent 1-μg cosyntropin testing. Baseline cortisol (mean difference -2.0 μg/dl, P=0.04) and 30-minute stimulated cortisol (mean difference -3.73 μg/dl, P=0.001) were significantly lower in patients with bronchiectasis. One patient had absolute adrenal insufficiency and 39.5 per cent (15/38) patients with bronchiectasis had impaired stimulated responses. Baseline and stimulated cortisol responses were unaffected by inhaled steroids (O.R 1.03, P=0.96). SGRQ scores were negatively correlated with body mass (r= -0.51, P=0.001) and bronchiectasis severity (r=0.37, P=0.019), but not related to baseline or stimulated cortisol responses.
Interpretation & conclusions: Our results showed that the impaired adrenal responses to 1-μg cosyntropin were common in patients with bronchiectasis. This was not associated with the use of inhaled steroids or severity of bronchiectasis. Poor health status was associated with advanced disease and not with cortisol responses to the 1-μg cosyntropin test.
Figures
Similar articles
-
Diagnosis of adrenal insufficiency in severe sepsis and septic shock.Am J Respir Crit Care Med. 2006 Dec 15;174(12):1319-26. doi: 10.1164/rccm.200509-1369OC. Epub 2006 Sep 14. Am J Respir Crit Care Med. 2006. PMID: 16973979
-
Total and free cortisol levels during 1 μg, 25 μg, and 250 μg cosyntropin stimulation tests compared to insulin tolerance test: results of a randomized, prospective, pilot study.Endocrine. 2017 Sep;57(3):388-393. doi: 10.1007/s12020-017-1371-9. Epub 2017 Jul 20. Endocrine. 2017. PMID: 28730418 Clinical Trial.
-
Cosyntropin-Stimulated Serum Free Cortisol in Healthy, Adrenally Insufficient, and Mildly Cirrhotic Populations.J Clin Endocrinol Metab. 2016 Mar;101(3):1075-81. doi: 10.1210/jc.2015-2285. Epub 2015 Dec 8. J Clin Endocrinol Metab. 2016. PMID: 26647150 Free PMC article.
-
Assessing effects of inhaled antibiotics in adults with non-cystic fibrosis bronchiectasis--experiences from recent clinical trials.Expert Rev Respir Med. 2018 Sep;12(9):769-782. doi: 10.1080/17476348.2018.1503540. Epub 2018 Aug 3. Expert Rev Respir Med. 2018. PMID: 30025482 Review.
-
Pitfalls in the interpretation of the cosyntropin stimulation test for the diagnosis of adrenal insufficiency.Curr Opin Endocrinol Diabetes Obes. 2019 Jun;26(3):139-145. doi: 10.1097/MED.0000000000000473. Curr Opin Endocrinol Diabetes Obes. 2019. PMID: 30855285 Review.
Cited by
-
Metabolomics analysis identifies novel plasma biomarkers of cystic fibrosis pulmonary exacerbation.Pediatr Pulmonol. 2015 Sep;50(9):869-77. doi: 10.1002/ppul.23225. Epub 2015 Jun 26. Pediatr Pulmonol. 2015. PMID: 26115542 Free PMC article.
-
Inhaled corticosteroids and secondary adrenal insufficiency.Open Respir Med J. 2014 Jan 31;8:93-100. doi: 10.2174/1874306401408010093. eCollection 2014. Open Respir Med J. 2014. PMID: 25674179 Free PMC article.
-
Adrenal reserve in acute exacerbation of non-cystic fibrosis bronchiectasis.Indian J Med Res. 2015 Dec;142(6):763-7. doi: 10.4103/0971-5916.174572. Indian J Med Res. 2015. PMID: 26831426 Free PMC article. No abstract available.
-
Adrenal Insufficiency in Cystic Fibrosis: A Rare Phenomenon?Can Respir J. 2018 Mar 13;2018:3629031. doi: 10.1155/2018/3629031. eCollection 2018. Can Respir J. 2018. PMID: 29731953 Free PMC article.
References
-
- Pasteur MC, Bilton D, Hill AT British Thoracic Society Non CF Bronchiectasis Guideline Group. British thoracic society guideline for non-CF bronchiectasis. Thorax. 2010;65:577. - PubMed
-
- Kapur N, Bell S, Kolbe J, Chang AB. Inhaled steroids for bronchiectasis. Cochrane Database Syst Rev. 2009;1:CD000996. - PubMed
-
- Hester KL, Macfarlane JG, Tedd H, Jary H, McAlinden P, Rostron L, et al. Fatigue in bronchiectasis. QJM. 2012;105:235–40. - PubMed
-
- Donnelly R, Williams KM, Baker AB, Badcock CA, Day RO, Seale JP. Effects of budesonide and fluticasone on 24-hour plasma cortisol. A dose-response study. Am J Respir Crit Care Med. 1997;156:1746–51. - PubMed
-
- Holme J, Tomlinson JW, Stockley RA, Stewart PM, Barlow N, Sullivan AL. Adrenal suppression in bronchiectasis and the impact of inhaled corticosteroids. Eur Respir J. 2008;32:1047–52. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical