

The nonallergic asthma of obesity. A matter of distal lung compliance
- PMID: 24821412
- PMCID: PMC4226017
- DOI: 10.1164/rccm.201401-0178OC
The nonallergic asthma of obesity. A matter of distal lung compliance
Abstract
Rationale: The pathogenesis of asthma in obesity is poorly understood, but may be related to breathing at low lung volumes.
Objectives: To determine if lung function in obese patients with asthma and control subjects would respond differently to weight loss.
Methods: Lung function was evaluated by conventional clinical tests and by impulse oscillometry in female late-onset, nonallergic patients with asthma and control subjects before, and 12 months after, bariatric surgery.
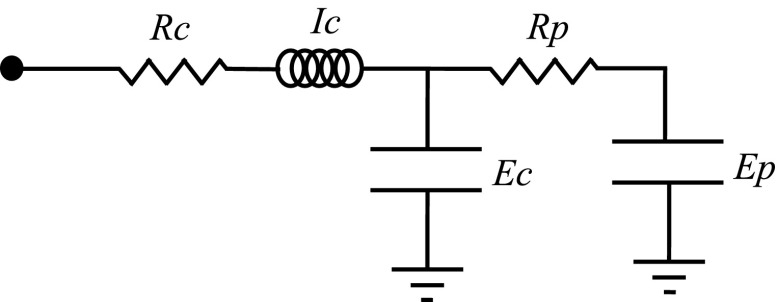
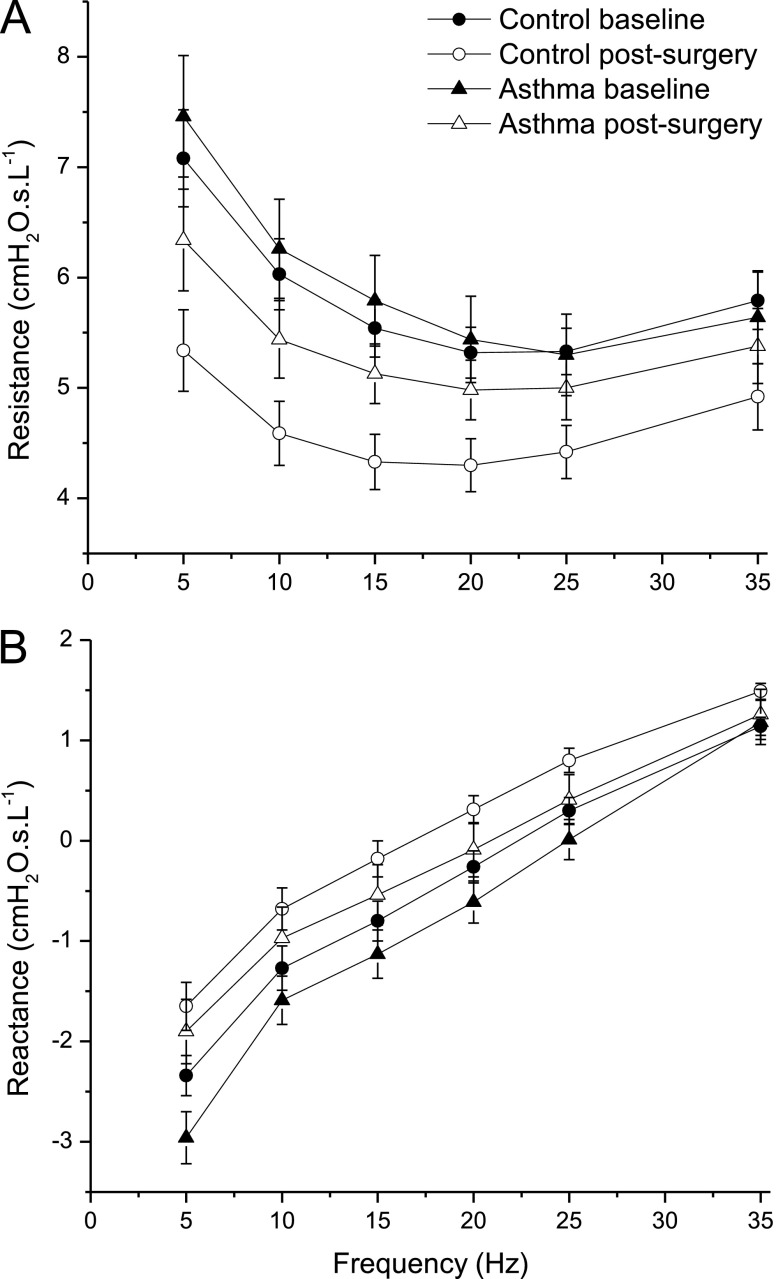
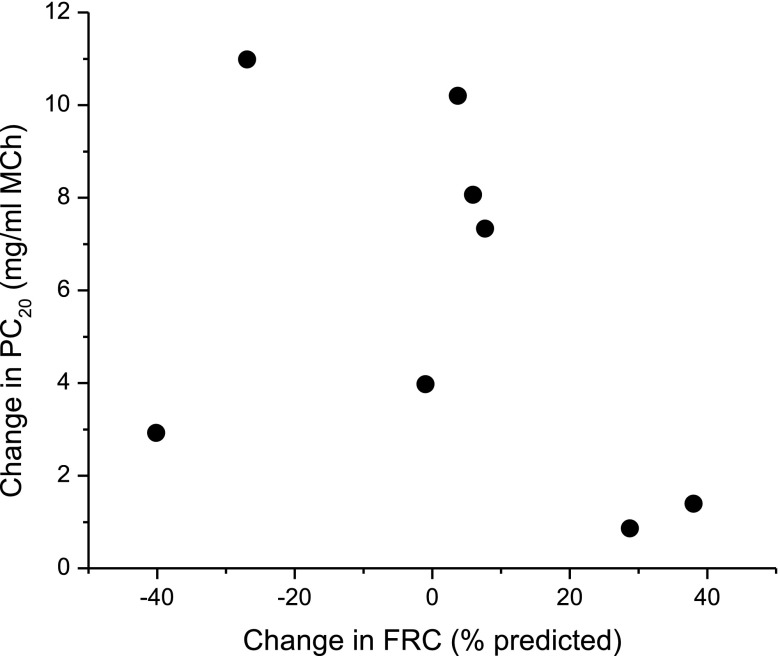
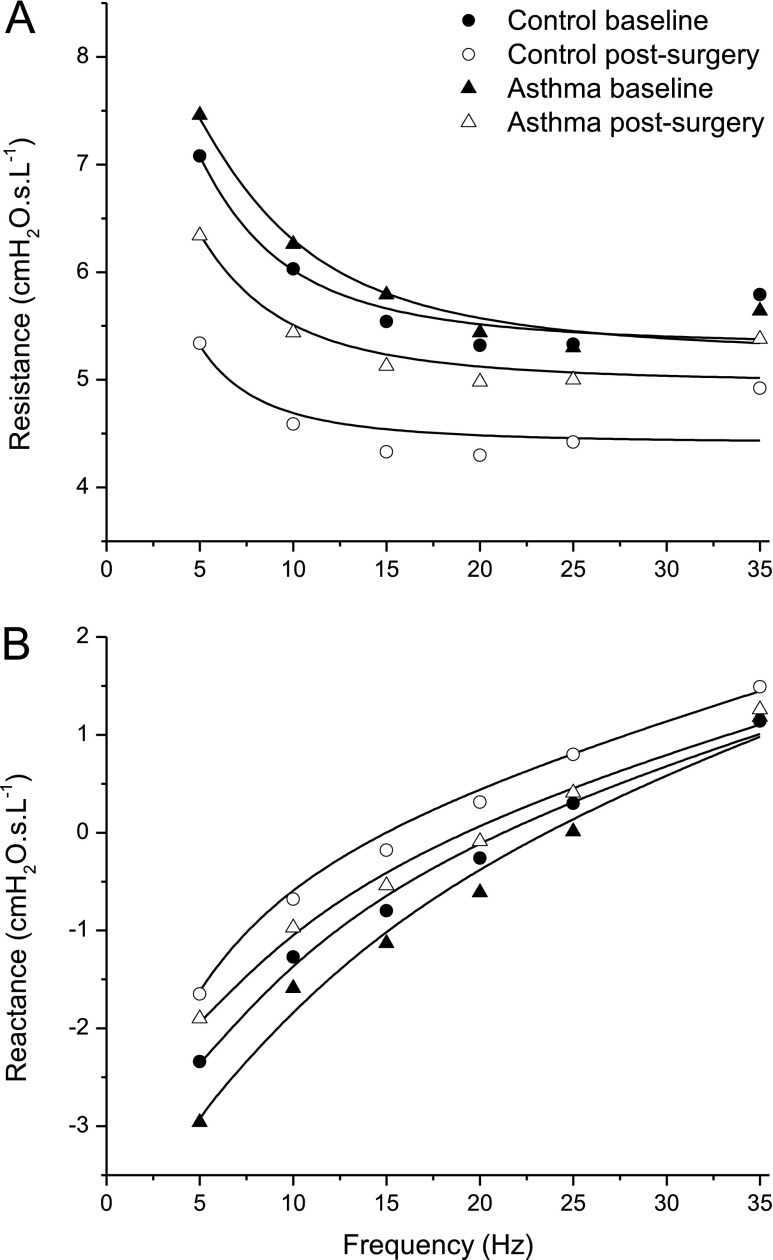
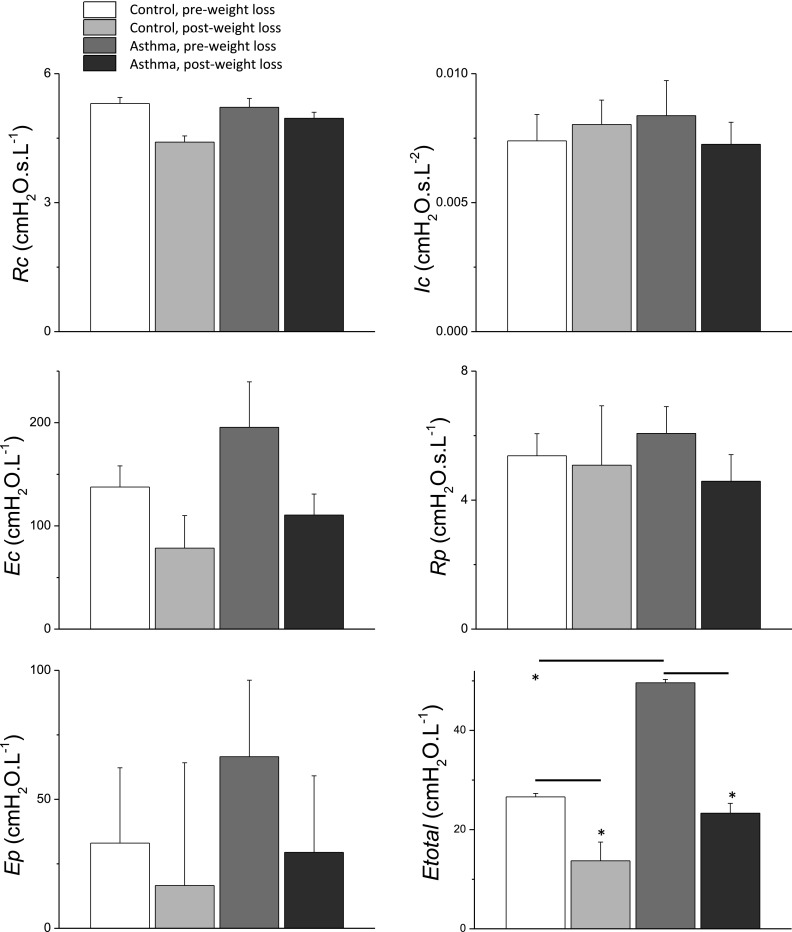
Measurements and main results: Patients with asthma (n = 10) had significantly lower FEV1 (79.8 ± 10.6 vs. 95.5 ± 7.0%) and FVC (82.4 ± 13.2 vs. 93.7 ± 8.9%) compared with control subjects (n = 13). There were no significant differences in FRC or TLC at baseline. Twelve months after surgery, control subjects had significant increases in FEV1 (95.5 ± 7.0 to 100.7 ± 5.9), FVC (93.6 ± 8.9 to 98.6 ± 8.3%), FRC (45.4 ± 18.5 to 62.1 ± 15.3%), and TLC (84.8 ± 15.0 to 103.1 ± 15.3%), whereas patients with asthma had improvement only in FEV1 (79.8 ± 10.6 to 87.2 ± 11.5). Control subjects and patients with asthma had a significantly different change in respiratory system resistance with weight loss: control subjects exhibited a uniform decrease in respiratory system resistance at all frequencies, whereas patients with asthma exhibited a decrease in frequency dependence of resistance. Fits of a mathematical model of lung mechanics to these impedance spectra suggest that the lung periphery was more collapsed by obesity in patients with asthma compared with control subjects.
Conclusions: Weight loss decompresses the lung in both obese control subjects and patients with asthma, but the more pronounced effects of weight loss on lung elastance suggest that the distal lung is inherently more collapsible in people with asthma.
Keywords: bariatric surgery; forced oscillation technique; impedance; lung volume.
Figures
Comment in
-
Obesity and asthma: "What we've got here is failure to communicate".Am J Respir Crit Care Med. 2014 Jun 15;189(12):i-ii. doi: 10.1164/rccm.201405-0989ED. Am J Respir Crit Care Med. 2014. PMID: 24930541 No abstract available.
References
-
- Chen Y, Dales R, Jiang Y. The association between obesity and asthma is stronger in nonallergic than allergic adults. Chest. 2006;130:890–895. - PubMed
-
- Dixon AE, Holguin F, Sood A, Salome CM, Pratley RE, Beuther DA, Celedón JC, Shore SA American Thoracic Society Ad Hoc Subcommittee on Obesity and Lung Disease. An official American Thoracic Society Workshop report: obesity and asthma. Proc Am Thorac Soc. 2010;7:325–335. - PubMed
-
- Taylor B, Mannino D, Brown C, Crocker D, Twum-Baah N, Holguin F. Body mass index and asthma severity in the National Asthma Survey. Thorax. 2008;63:14–20. - PubMed
-
- Mosen DM, Schatz M, Magid DJ, Camargo CA., JrThe relationship between obesity and asthma severity and control in adults. J Allergy Clin Immunol2008. 122:507–511, e6 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
