

Review
doi: 10.2174/1573403x10666140513103709.
The vernakalant story: how did it come to approval in Europe and what is the delay in the U.S.A?
Affiliations
- PMID: 24821654
- PMCID: PMC4101194
- DOI: 10.2174/1573403x10666140513103709
Item in Clipboard
Review
The vernakalant story: how did it come to approval in Europe and what is the delay in the U.S.A?
Curr Cardiol Rev.
2014 Nov.
Abstract
The sudden onset of atrial fibrillation (AF) is often associated with rapid irregular palpitations, chest pain, shortness of breath and considerable anxiety. If a patient presents shortly after the onset of the arrhythmia the physician may adopt initially an expectant "wait and see" policy, perhaps with the help of mild sedation and drug therapy to reduce the ventricular rate. If the arrhythmia does not terminate spontaneously and has been present for less than 24-48 hours restoration of sinus rhythm by cardioversion should be considered. This manuscript reviews the option of electrical cardioversion versus pharmacologic and the data for, the role of, and the status of vernakalant with respect to the latter.
Figures
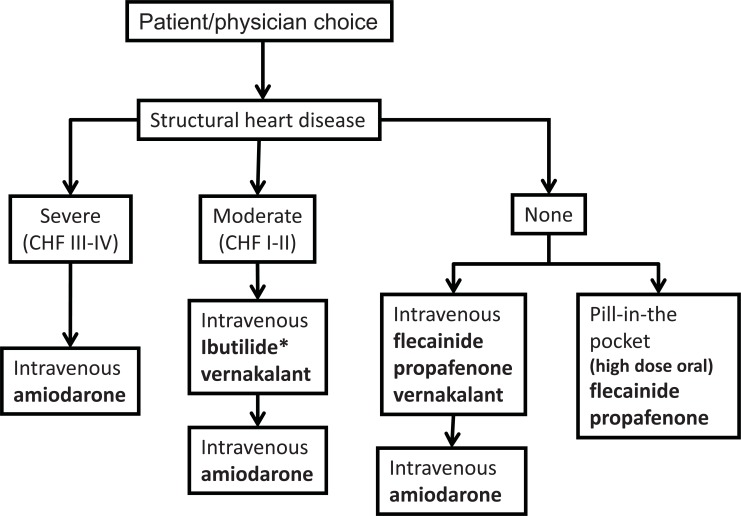
Choice of pharmacological agent for cardioversion in an acute setting. Choice of an antiarrhythmic drug is dependent on availability and underlying structural heart disease. Optimum drug choices are indicated in bold. CHF = congestive heart failure.
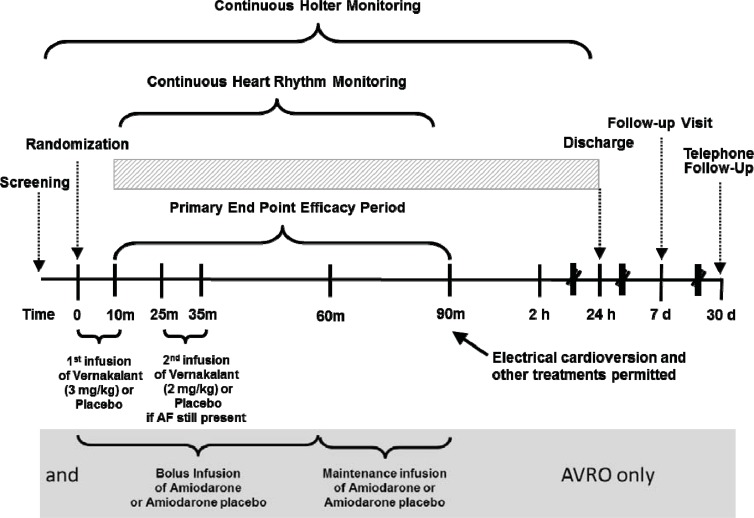
Schematic of the clinical trials for the development of vernakalant. All trial used sinus rhythm at 90 minutes after the start of the vernakalant infusion as the primary endpoint. In CRAFT the infusion doses were reversed. In CRAFT, ACT I, II and III patients were randomised to blinded vernakalant or placebo. In AVRO patients received either amiodarone or vernakalant (or appropriate placebos) in a in a double-blind, double-dummy design. ACT IV was not controlled, but contributed to the safety database of vernakalant.
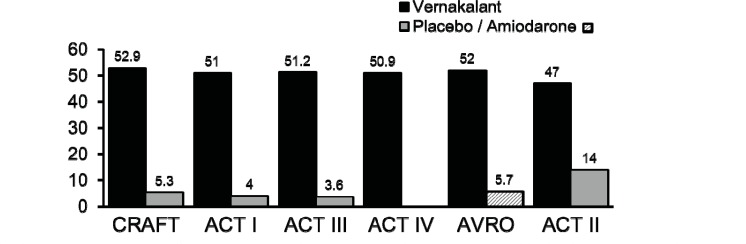
Termination of recent onset AF following intravenous infusion of vernakalant compared with placebo (ACT I, II and III) or amiodarone
(AVRO). The median time to termination was between 8 and14 minutes. 75-80% converted after the first dose.
References
-
- EU Summary of Product Characteristics. BRINAVESS MSD. 2010
-
- de Riva-Silva M, Montero-Cabezas JM, Salgado-Aranda R, López-Gil M, Fontenla-Cerezuela A, Arribas-Ynsaurriaga F. 1:1 Atrial Flutter After Vernakalant Administration for Atrial Fibrillation Cardioversion. Rev Esp Cardiol. 2012;65(11):1062–4. - PubMed
-
- Bash LD, Buono JL, Davies GM , et al. Systematic review and meta-analysis of the efficacy of cardioversion by vernakalant and comparators in patients with atrial fibrillation. Cardiovasc Drugs Ther. 2012;26(2):167–79. - PubMed
-
- Burashnikov A, Pourrier M, Gibson JK, Lynch JJ, Antzelevitch C. Rate-dependent effects of vernakalant in the isolated non-remodeled canine left atria are primarily due to block of the sodium channel: comparison with ranolazine and dl-sotalol. Circ Arrhythm Electrophysiol. 2012;5(2):400–8. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
