

After 2015: infectious diseases in a new era of health and development
- PMID: 24821913
- PMCID: PMC4024220
- DOI: 10.1098/rstb.2013.0426
After 2015: infectious diseases in a new era of health and development
Abstract
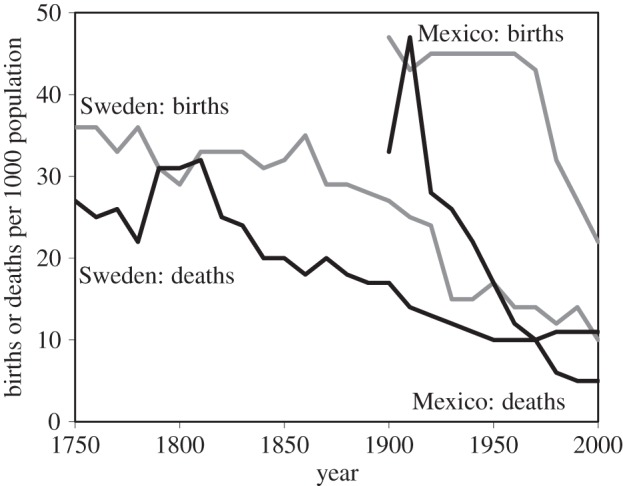
Running over timescales that span decades or centuries, the epidemiological transition provides the central narrative of global health. In this transition, a reduction in mortality is followed by a reduction in fertility, creating larger, older populations in which the main causes of illness and death are no longer acute infections of children but chronic diseases of adults. Since the year 2000, the Millennium Development Goals (MDGs) have provided a framework for accelerating the decline of infectious diseases, backed by a massive injection of foreign investment to low-income countries. Despite the successes of the MDGs era, the inhabitants of low-income countries still suffer an enormous burden of disease owing to diarrhoea, pneumonia, HIV/AIDS, tuberculosis, malaria and other pathogens. Adding to the predictable burden of endemic disease, the threat of pandemics is ever-present and global. With a view to the future, this review spotlights five aspects of the fight against infection beyond 2015, when the MDGs will be replaced by a new set of goals for poverty reduction and sustainable development. These aspects are: exploiting the biological links between infectious and non-infectious diseases; controlling infections among the new urban majority; enhancing the response to international health threats; expanding childhood immunization programmes to prevent acute and chronic diseases in adults; and working towards universal health coverage. By scanning the wider horizon now, infectious disease specialists have the chance to shape the post-2015 era of health and development.
Keywords: Millennium Development Goals; Universal Health Coverage.
Figures






References
-
- Population Reference Bureau Staff. 2004. Transitions in world population. Popul. Bull. 59, 1–40.
-
- World Health Organization. 2013. Mortality and global health estimates. Geneva, Switzerland: World Health Organization.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical