

The ongoing challenge of latent tuberculosis
- PMID: 24821923
- PMCID: PMC4024230
- DOI: 10.1098/rstb.2013.0437
The ongoing challenge of latent tuberculosis
Abstract
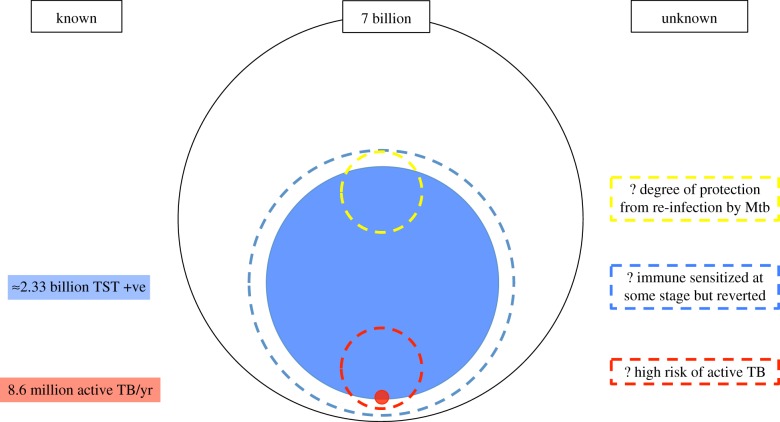
The global health community has set itself the task of eliminating tuberculosis (TB) as a public health problem by 2050. Although progress has been made in global TB control, the current decline in incidence of 2% yr(-1) is far from the rate needed to achieve this. If we are to succeed in this endeavour, new strategies to reduce the reservoir of latently infected persons (from which new cases arise) would be advantageous. However, ascertainment of the extent and risk posed by this group is poor. The current diagnostics tests (tuberculin skin test and interferon-gamma release assays) poorly predict who will develop active disease and the therapeutic options available are not optimal for the scale of the intervention that may be required. In this article, we outline a basis for our current understanding of latent TB and highlight areas where innovation leading to development of novel diagnostic tests, drug regimens and vaccines may assist progress. We argue that the pool of individuals at high risk of progression may be significantly smaller than the 2.33 billion thought to be immune sensitized by Mycobacterium tuberculosis and that identifying and targeting this group will be an important strategy in the road to elimination.
Keywords: Mycobacterium tuberculosis; diagnosis; elimination; latent tuberculosis; natural history; treatment.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical