

Diagnostic and prognostic significance of lysophosphatidic acid in malignant pleural effusions
- PMID: 24822107
- PMCID: PMC4014993
- DOI: 10.3978/j.issn.2072-1439.2014.02.14
Diagnostic and prognostic significance of lysophosphatidic acid in malignant pleural effusions
Abstract
Background: Lysophosphatidic acid (LPA) is an important extracellular signal transmitter and intracellular second messenger in body fluids. It can be detected in the ascitic fluid of patients with ovarian cancer. Increasing evidence shows that LPA can stimulate cancer cell proliferation and promote tumor invasion and metastasis. Our study aimed to evaluate the diagnostic value of LPA in differentiating between malignant pleural effusions (MPEs) and benign pleural effusions (BPEs) and to evaluate the association between the level of LPA in MPE and the prognosis of lung cancer patients.
Patients and methods: The level of LPA in the pleural effusions (PEs) of 123 patients (94 MPE, 29 BPE) with lung cancer was evaluated using an enzyme-linked immunosorbent assay. The performance of LPA was analyzed by standard Receiver operator characteristic curve (ROC) analysis methods, using the area under the curve (AUC) as a measure of accuracy. Overall survival (OS) curves and progression-free survival (PFS) curves were based on the Kaplan-Meier method, and the survival differences between subgroups were analyzed using the log-rank or Breslow test (SPSS software). A multivariate Cox proportional hazards model was used to assess whether LPA independently predicted lung cancer survival.
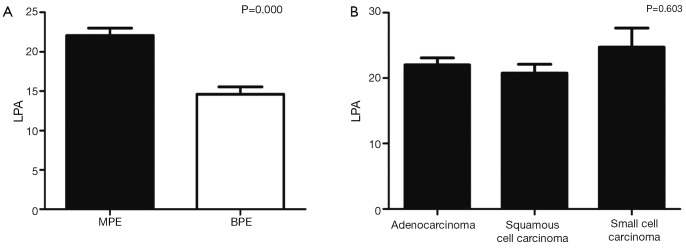
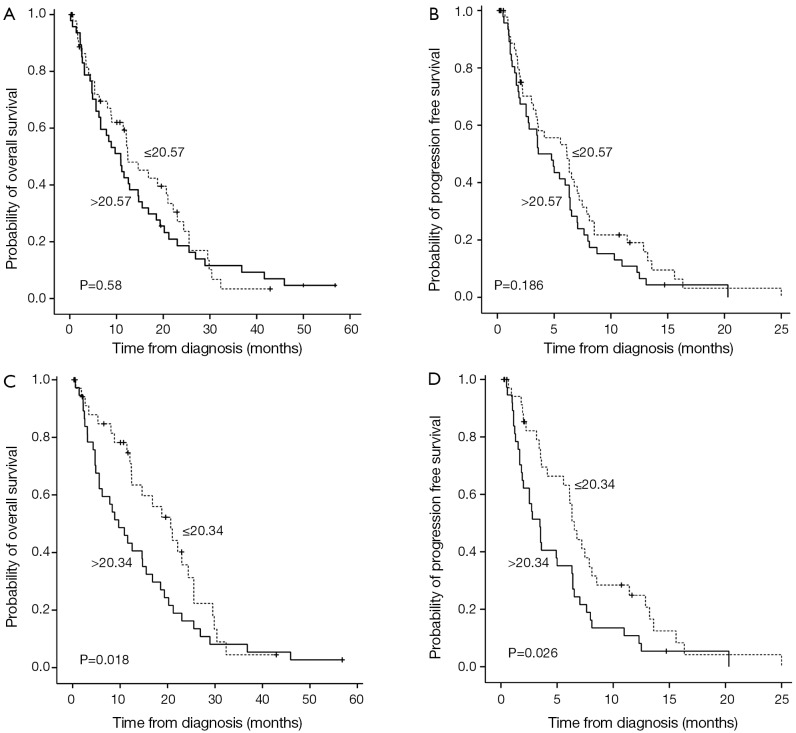
Results: The levels of LPA differed significantly between MPE (22.08±8.72 µg/L) and BPE (14.61±5.12 µg/L) (P<0.05). Using a cutoff point of 18.93 µg/L, LPA had a sensitivity of 60% and a specificity of 83% to distinguish MPEs from BPEs with an AUC of 0.769±0.045 (SE) (P=0.000) (95% CI, 0.68-0.857). In the three pathological types of lung cancer patients with MPE, there were no significant associations between LPA levels and the length of PFS and OS (P=0.58 and 0.186, respectively). Interestingly, in the patients with MPE caused by lung adenocarcinoma there were significant associations between the LPA levels and the PFS and OS (P=0.018 and 0.026, respectively). Multivariate analysis showed that the LPA level was an independent prognostic factor for PFS in lung adenocarcinoma.
Conclusions: Our results indicate that LPA can be used as a new biomarker for the diagnosis of MPE caused by lung cancer and that higher levels of LPA are related to shorter PFS in adenocarcinoma of the lung.
Keywords: Lysopohsphatidic acid (LPA); diagnosis; lung cancer; malignant pleural effusions (MPEs); prognosis.
Figures

Similar articles
-
Diagnostic and prognostic values of endothelial-cell-specific molecule-1 with malignant pleural effusions in patients with non-small cell lung cancer.Oncotarget. 2017 Jul 25;8(30):49217-49223. doi: 10.18632/oncotarget.17455. Oncotarget. 2017. PMID: 28514746 Free PMC article.
-
Diagnostic Value of Circulating Extracellular miR-134, miR-185, and miR-22 Levels in Lung Adenocarcinoma-Associated Malignant Pleural Effusion.Cancer Res Treat. 2014 Apr;46(2):178-85. doi: 10.4143/crt.2014.46.2.178. Epub 2014 Apr 22. Cancer Res Treat. 2014. PMID: 24851110 Free PMC article.
-
Diagnostic accuracy of endostatin for malignant pleural effusion: A clinical study and meta-analysis.Postgrad Med. 2015 Jun;127(5):529-34. doi: 10.1080/00325481.2015.1048180. Epub 2015 May 15. Postgrad Med. 2015. PMID: 25979108
-
Evaluation of predictive value of pleural CEA in patients with pleural effusions and histological findings: A prospective study and literature review.Clin Biochem. 2016 Nov;49(16-17):1227-1231. doi: 10.1016/j.clinbiochem.2016.08.006. Epub 2016 Aug 10. Clin Biochem. 2016. PMID: 27521620 Review.
-
The Value of Cytology in the Evaluation of Malignant Pericardial Effusions: A Systematic Review.Diagnostics (Basel). 2022 Feb 1;12(2):367. doi: 10.3390/diagnostics12020367. Diagnostics (Basel). 2022. PMID: 35204458 Free PMC article. Review.
Cited by
-
Activity and clinical relevance of autotaxin and lysophosphatidic acid pathways in high-grade serous carcinoma.Virchows Arch. 2018 Oct;473(4):463-470. doi: 10.1007/s00428-018-2418-x. Epub 2018 Jul 21. Virchows Arch. 2018. PMID: 30032361
-
LPA3 is a precise therapeutic target and potential biomarker for ovarian cancer.Med Oncol. 2022 Jan 4;39(2):17. doi: 10.1007/s12032-021-01616-5. Med Oncol. 2022. PMID: 34982278
-
Diverse Effects of Lysophosphatidic Acid Receptors on Ovarian Cancer Signaling Pathways.J Oncol. 2019 Sep 17;2019:7547469. doi: 10.1155/2019/7547469. eCollection 2019. J Oncol. 2019. PMID: 31636669 Free PMC article.
-
Lysophospholipid Signaling in the Epithelial Ovarian Cancer Tumor Microenvironment.Cancers (Basel). 2018 Jul 9;10(7):227. doi: 10.3390/cancers10070227. Cancers (Basel). 2018. PMID: 29987226 Free PMC article. Review.
-
Promising pharmacological directions in the world of lysophosphatidic Acid signaling.Biomol Ther (Seoul). 2015 Jan;23(1):1-11. doi: 10.4062/biomolther.2014.109. Epub 2015 Jan 1. Biomol Ther (Seoul). 2015. PMID: 25593637 Free PMC article. Review.
References
-
- American Thoracic Society Management of malignant pleural effusions. Am J Respir Crit Care Med 2000;162:1987-2001 - PubMed
-
- Stathopoulos GT, Psallidas I, Moustaki A, et al. A central role for tumor-derived monocyte chemoattractant protein-1 in malignant pleural effusion. J Natl Cancer Inst 2008;100:1464-76 - PubMed
-
- Martínez-Moragón E, Aparicio J, Sanchis J, et al. Malignant pleural effusion: prognostic factors for survival and response to chemical pleurodesis in a series of 120 cases. Respiration 1998;65:108-13 - PubMed
-
- Yoneda KY, Mathur PN, Gasparini S. The evolving role of interventional pulmonary in the interdisciplinary approach to the staging and management of lung cancer. Part III: diagnosis and management of malignant pleural effusions. Clin Lung Cancer 2007;8:535-47 - PubMed
-
- Naito T, Satoh H, Ishikawa H, et al. Pleural effusion as a significant prognostic factor in non-small cell lung cancer. Anticancer Res 1997;17:4743-6 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous