

Visualizing typical features of breast fibroadenomas using phase-contrast CT: an ex-vivo study
- PMID: 24824169
- PMCID: PMC4019647
- DOI: 10.1371/journal.pone.0097101
Visualizing typical features of breast fibroadenomas using phase-contrast CT: an ex-vivo study
Abstract
Background: Fibroadenoma is the most common benign solid breast lesion type and a very common cause for histologic assessment. To justify a conservative therapy, a highly specific discrimination between fibroadenomas and other breast lesions is crucial. Phase-contrast imaging offers improved soft-tissue contrast and differentiability of fine structures combined with the potential of 3-dimensional imaging. In this study we assessed the potential of grating-based phase-contrast CT imaging for visualizing diagnostically relevant features of fibroadenomas.
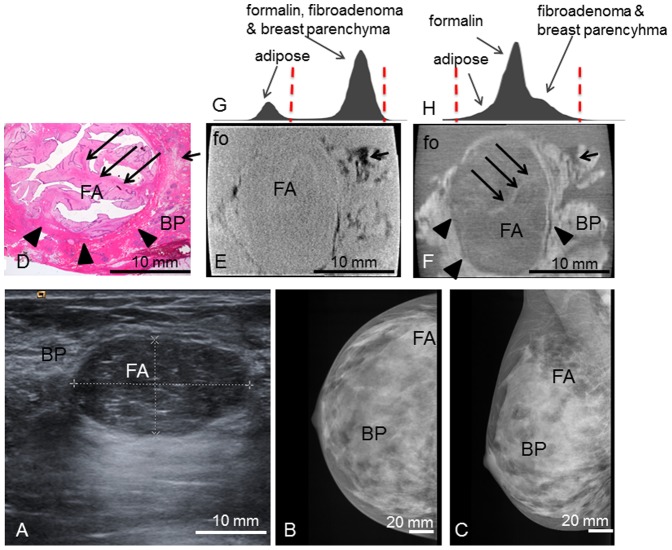
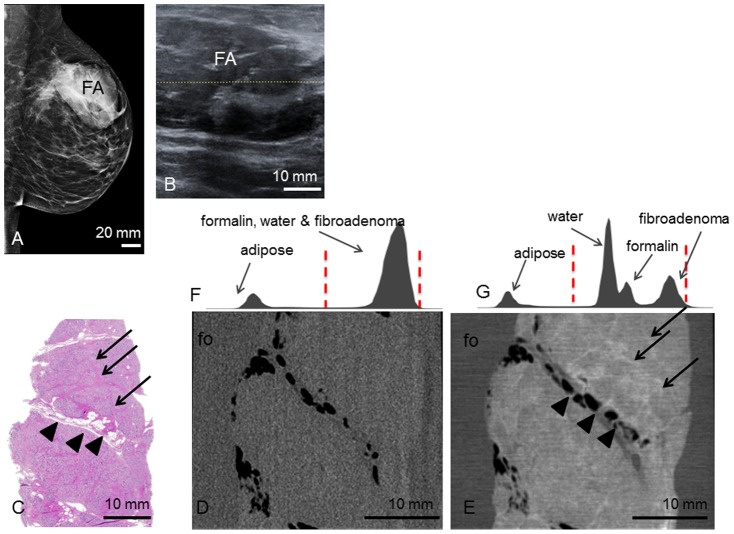
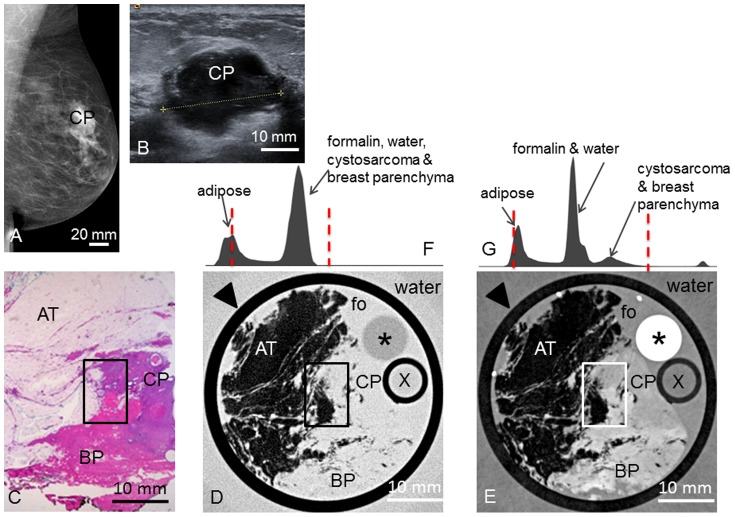
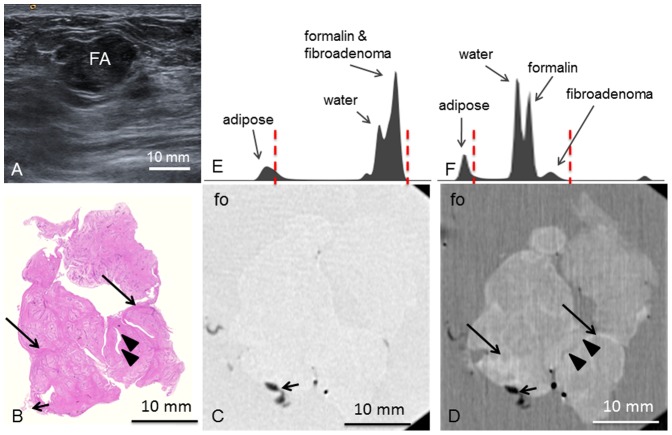
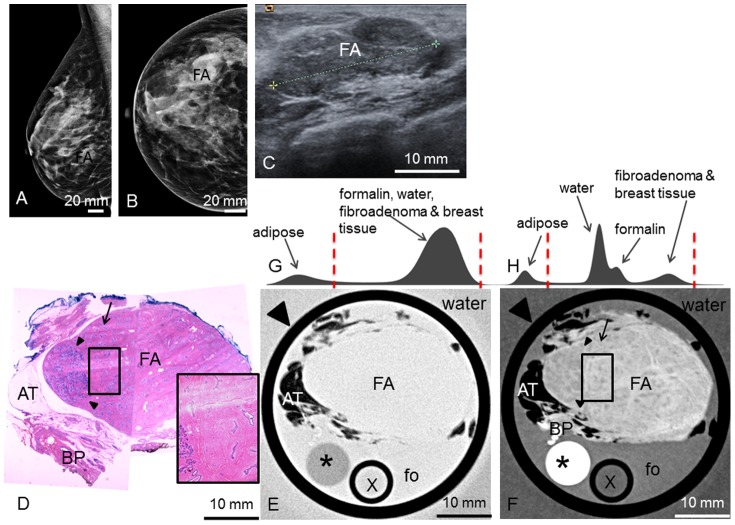
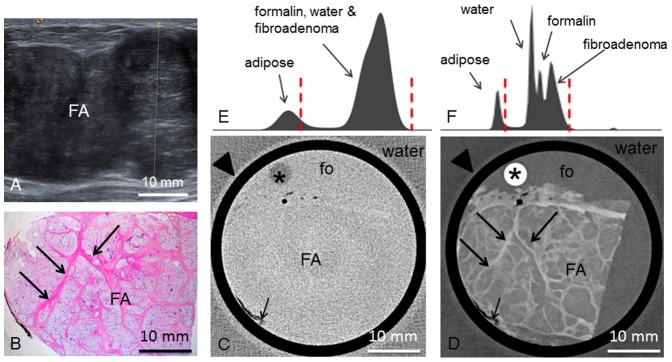
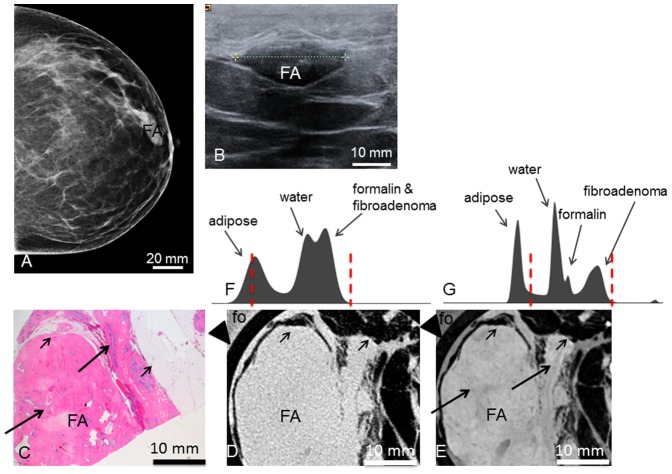
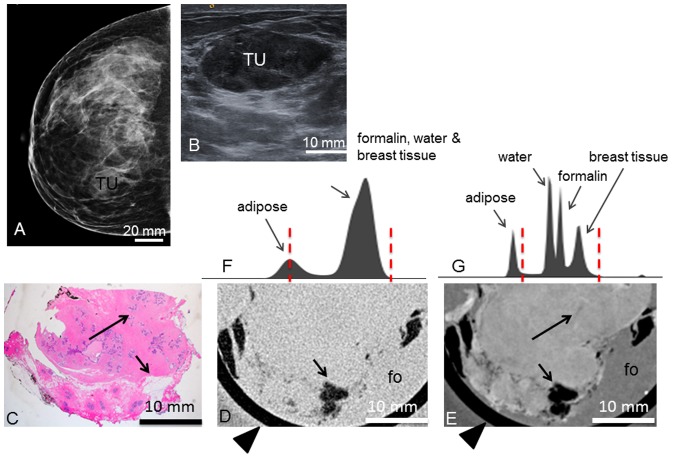
Materials and methods: Grating-based phase-contrast CT was performed on six ex-vivo formalin-fixed breast specimens containing a fibroadenoma and three samples containing benign changes that resemble fibroadenomas using Talbot Lau interferometry and a polychromatic X-ray source. Phase-contrast and simultaneously acquired absorption-based 3D-datasets were manually matched with corresponding histological slices. The visibility of diagnostically valuable features was assessed in comparison with histology as the gold-standard.
Results: In all cases, matching of grating-based phase-contrast CT images and histology was successfully completed. Grating-based phase-contrast CT showed greatly improved differentiation of fine structures and provided accurate depiction of strands of fibrous tissue within the fibroadenomas as well as of the diagnostically valuable dilated, branched ductuli of the fibroadenomas. A clear demarcation of tumor boundaries in all cases was provided by phase- but not absorption-contrast CT.
Conclusions: Pending successful translation of the technology to a clinical setting and considerable reduction of the required dose, the data presented here suggest that grating-based phase-contrast CT may be used as a supplementary non-invasive diagnostic tool in breast diagnostics. Phase-contrast CT may thus contribute to the reduction of false positive findings and reduce the recall and core biopsy rate in population-based screening. Phase-contrast CT may further be used to assist during histopathological workup, offering a 3D view of the tumor and helping to identify diagnostically valuable tissue sections within large tumors.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of phase-contrast CT of breast tissue at conventional X-ray sources - presentation of selected findings.Z Med Phys. 2013 Sep;23(3):212-21. doi: 10.1016/j.zemedi.2013.02.005. Epub 2013 Mar 11. Z Med Phys. 2013. PMID: 23489931
-
Assessment of intraductal carcinoma in situ (DCIS) using grating-based X-ray phase-contrast CT at conventional X-ray sources: An experimental ex-vivo study.PLoS One. 2019 Jan 9;14(1):e0210291. doi: 10.1371/journal.pone.0210291. eCollection 2019. PLoS One. 2019. PMID: 30625220 Free PMC article.
-
Grating-based x-ray dark-field mammography: Assessing complementary imaging information in simple cystic lesions and typical fibroadenoma.Med Phys. 2025 Apr;52(4):2145-2154. doi: 10.1002/mp.17603. Epub 2025 Jan 3. Med Phys. 2025. PMID: 39752625 Free PMC article.
-
Assessment of grating-based X-ray phase-contrast CT for differentiation of invasive ductal carcinoma and ductal carcinoma in situ in an experimental ex vivo set-up.Eur Radiol. 2013 Feb;23(2):381-7. doi: 10.1007/s00330-012-2592-1. Epub 2012 Aug 31. Eur Radiol. 2013. PMID: 22932738 Review.
-
Fibroadenomas in adolescence.Curr Opin Obstet Gynecol. 2009 Oct;21(5):402-6. doi: 10.1097/GCO.0b013e32832fa06b. Curr Opin Obstet Gynecol. 2009. PMID: 19606032 Review.
Cited by
-
Dedicated breast CT: state of the art-Part II. Clinical application and future outlook.Eur Radiol. 2022 Apr;32(4):2286-2300. doi: 10.1007/s00330-021-08178-0. Epub 2021 Sep 3. Eur Radiol. 2022. PMID: 34476564 Review.
-
Monochromatic breast computed tomography with synchrotron radiation: phase-contrast and phase-retrieved image comparison and full-volume reconstruction.J Med Imaging (Bellingham). 2019 Jul;6(3):031402. doi: 10.1117/1.JMI.6.3.031402. Epub 2018 Nov 27. J Med Imaging (Bellingham). 2019. PMID: 30525064 Free PMC article.
-
Experimental Realisation of High-sensitivity Laboratory X-ray Grating-based Phase-contrast Computed Tomography.Sci Rep. 2016 Apr 4;6:24022. doi: 10.1038/srep24022. Sci Rep. 2016. PMID: 27040492 Free PMC article.
-
Dose and spatial resolution analysis of grating-based phase-contrast mammography using an inverse Compton x-ray source.J Med Imaging (Bellingham). 2020 Mar;7(2):023505. doi: 10.1117/1.JMI.7.2.023505. Epub 2020 Apr 22. J Med Imaging (Bellingham). 2020. PMID: 32341937 Free PMC article.
-
Realistic wave-optics simulation of X-ray dark-field imaging at a human scale.Sci Rep. 2025 Jul 23;15(1):26748. doi: 10.1038/s41598-025-12047-x. Sci Rep. 2025. PMID: 40702112 Free PMC article.
References
-
- Pearlman MD, Griffin JL (2010) Benign breast disease. Obstet Gynecol 116: 747–758. - PubMed
-
- Weaver DL, Rosenberg RD, Barlow WE, Ichikawa L, Carney PA, et al. (2006) Pathologic findings from the Breast Cancer Surveillance Consortium: population-based outcomes in women undergoing biopsy after screening mammography. Cancer 106: 732–742. - PubMed
-
- Kerlikowske K, Smith-Bindman R, Ljung BM, Grady D (2003) Evaluation of abnormal mammography results and palpable breast abnormalities. Ann Intern Med 139: 274–284. - PubMed
-
- Tilanus-Linthorst M, Verhoog L, Obdeijn IM, Bartels K, Menke-Pluymers M, et al. (2002) A BRCA1/2 mutation, high breast density and prominent pushing margins of a tumor independently contribute to a frequent false-negative mammography. Int J Cancer 102: 91–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
