

Baseline characteristics predict risk of progression and response to combined medical therapy for benign prostatic hyperplasia (BPH)
- PMID: 24825577
- PMCID: PMC4231026
- DOI: 10.1111/bju.12802
Baseline characteristics predict risk of progression and response to combined medical therapy for benign prostatic hyperplasia (BPH)
Abstract
Objective: To better risk stratify patients, using baseline characteristics, to help optimise decision-making for men with moderate-to-severe lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) through a secondary analysis of the Medical Therapy of Prostatic Symptoms (MTOPS) trial.
Patients and methods: After review of the literature, we identified potential baseline risk factors for BPH progression. Using bivariate tests in a secondary analysis of MTOPS data, we determined which variables retained prognostic significance. We then used these factors in Cox proportional hazard modelling to: i) more comprehensively risk stratify the study population based on pre-treatment parameters and ii) to determine which risk strata stood to benefit most from medical intervention.
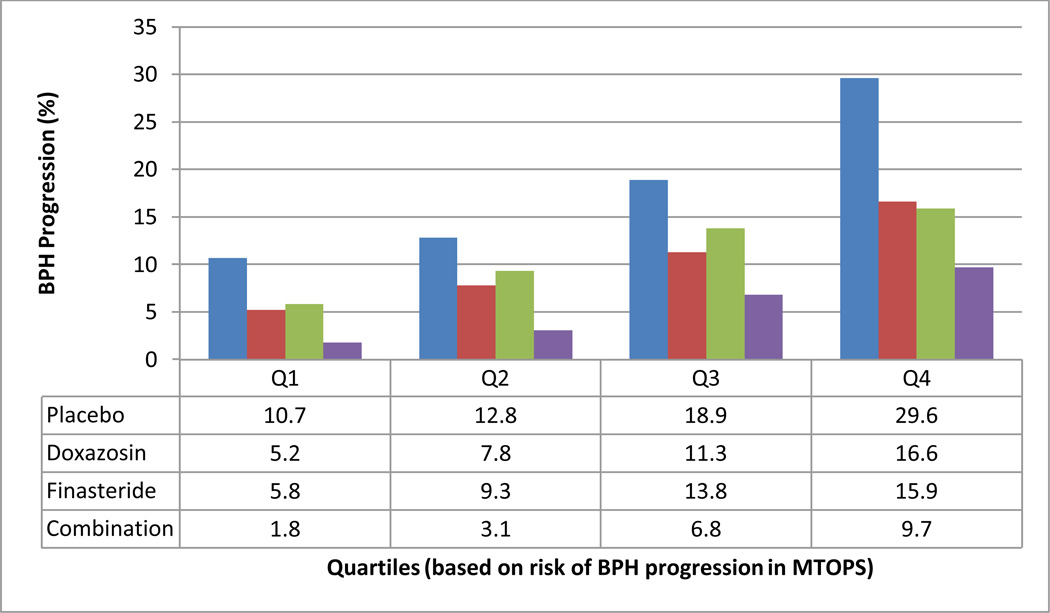
Results: In all, 3047 men were followed in MTOPS for a mean of 4.5 years. We found varying risks of progression across quartiles. Baseline BPH Impact Index score, post-void residual urine volume, serum prostate-specific antigen (PSA) level, age, American Urological Association Symptom Index score, and maximum urinary flow rate were found to significantly correlate with overall BPH progression in multivariable analysis.
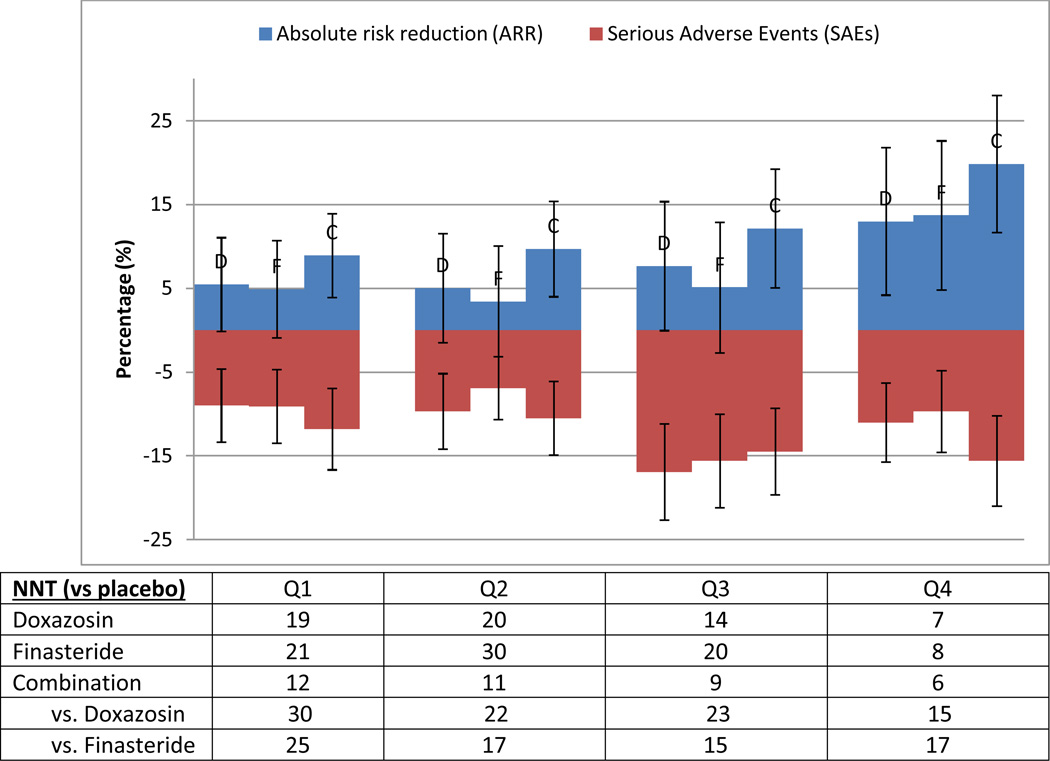
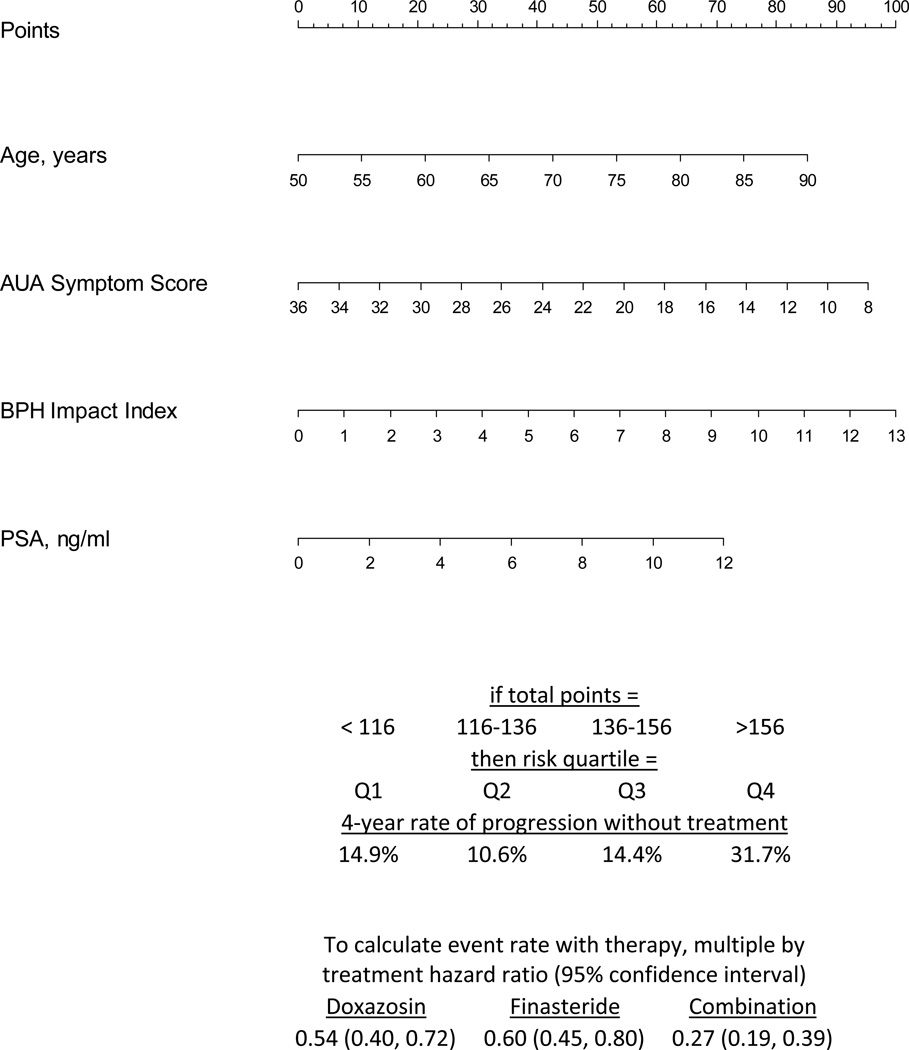
Conclusions: Using baseline factors permits estimation of individual patient risk for clinical progression and the benefits of medical therapy. A novel clinical decision tool based on these analyses will allow clinicians to weigh patient-specific benefits against possible risks of adverse effects for a given patient.
Keywords: benign prostatic hyperplasia (BPH); lower urinary tract symptoms (LUTS); risk factors.
© 2014 The Authors. BJU International © 2014 BJU International.
Conflict of interest statement
None of the four authors have any conflicts of interest.
Figures
References
-
- Flanigan RC, Reda DJ, Wasson JH, et al. 5-year outcome of surgical resection and watchful waiting for men with moderately symptomatic benign prostatic hyperplasia: a Department of Veterans Affairs cooperative study. J Urol. 1998;160(1):12–16. discussion 16-17. - PubMed
-
- Jacobsen SJ, Girman CJ, Lieber MM. Natural history of benign prostatic hyperplasia. Urology. 2001;58(6 Suppl 1):5–16. discussion 16. - PubMed
-
- Martin S, Lange K, Haren MT, et al. Risk factors for progression or improvement of lower urinary tract symptoms in a prospective cohort of men. J Urol. 2014;191(1):130–137. - PubMed
-
- Roehrborn CG. BPH progression: concept and key learning from MTOPS, ALTESS, COMBAT, and ALF-ONE. BJU Int. 2008;101(Suppl 3):17–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
