

Ventricular Septal Defect in an Octogenarian: A Case Report of VSD Surgical Repair Concomitant with Coronary Artery Bypass and Valvular Surgery
- PMID: 24826250
- PMCID: PMC4008348
- DOI: 10.1155/2012/429569
Ventricular Septal Defect in an Octogenarian: A Case Report of VSD Surgical Repair Concomitant with Coronary Artery Bypass and Valvular Surgery
Abstract
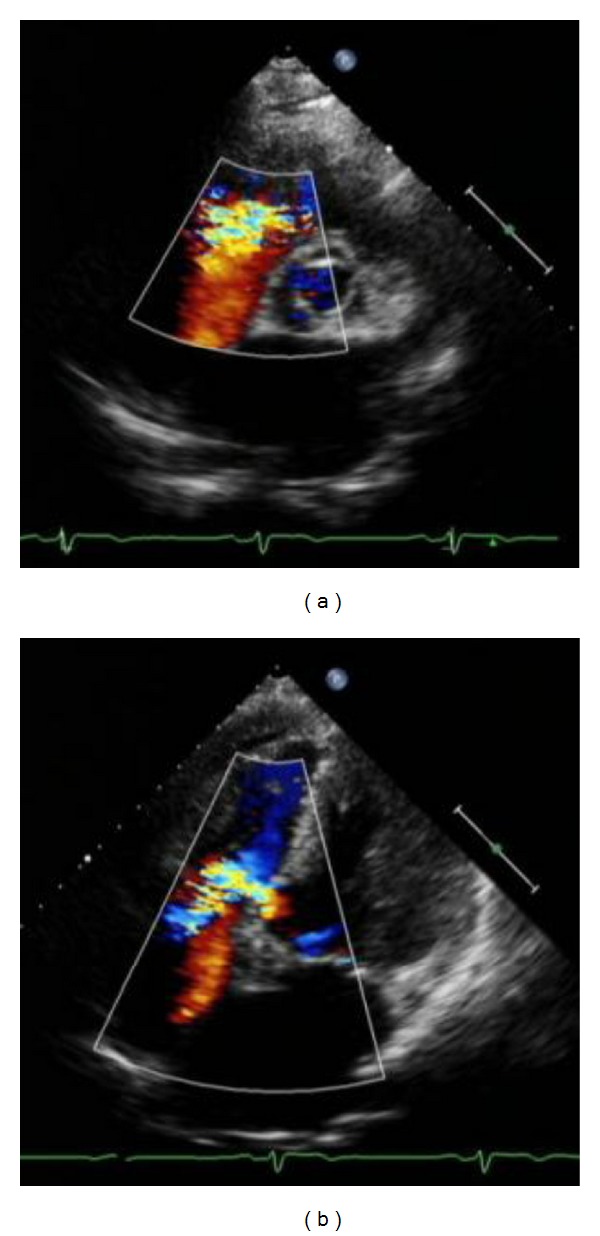
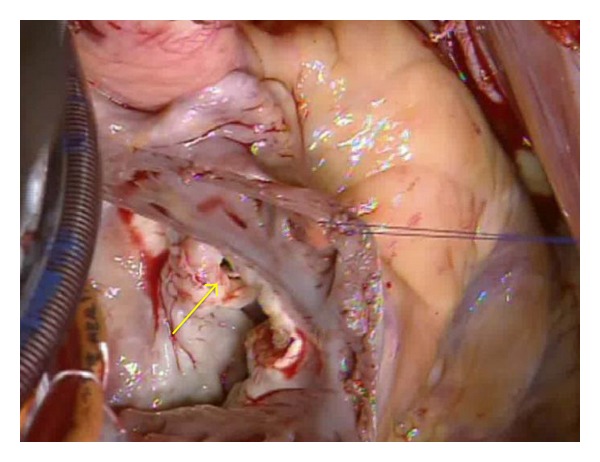
Finding an untreated or asymptomatic large ventricular septal defect (VSD) in an elderly patient is uncommon. The present case was an 81-year-old man who suffered from acute myocardial infarction due to three-vessel coronary disease, mitral and tricuspid valve insufficiency, and high-flow perimembranous VSD (Qp/Qs 2.3). Although the patient was elderly and the VSD had been asymptomatic for a long time, we considered that high-flow VSD and valve diseases should be repaired simultaneously with coronary disease. Then, he underwent elective surgery, namely, VSD patch repair concomitant with coronary artery bypass grafting, and mitral and tricuspid annuloplasty. His postoperative course was uneventful. We conclude that, even for an octogenarian, surgical repair of VSD is recommendable, if surgical indications are appropriate.
Figures

Similar articles
-
Closure of perimembranous ventricular septal defect using transcatheter technique versus surgical repair.Kardiol Pol. 2005 Dec;63(6):595-602; discussion 603-4. Kardiol Pol. 2005. PMID: 16380857
-
In patients undergoing surgical repair of post-infarction ventricular septal defect, does concomitant revascularization improve prognosis?Interact Cardiovasc Thorac Surg. 2009 Nov;9(5):879-87. doi: 10.1510/icvts.2009.210658. Epub 2009 Aug 19. Interact Cardiovasc Thorac Surg. 2009. PMID: 19692439 Review.
-
Concomitant pulmonary valve replacement, VSD closure and coronary artery bypass surgery.J Heart Valve Dis. 1998 Jan;7(1):117-20. J Heart Valve Dis. 1998. PMID: 9502149
-
Closure of isolated ventricular septal defect with detachment of the tricuspid valve.J Card Surg. 1995 Sep;10(5):564-8. doi: 10.1111/j.1540-8191.1995.tb00633.x. J Card Surg. 1995. PMID: 7488779
-
Repair of ischemic ventricular septal defect with and without coronary artery bypass grafting.J Card Surg. 2020 May;35(5):1062-1071. doi: 10.1111/jocs.14515. Epub 2020 Apr 1. J Card Surg. 2020. PMID: 32237166
References
-
- Perloff JK. The Clinical Recognition of Congenital Heart Disease. 4th edition. Philadelphia, Pa, USA: WB Saunders; 1994.
-
- Mahoney LT. Acyanotic congenital heart disease: atrial and ventricular septal defects, atrioventricular canal, patent ductus arteriosus, pulmonic stenosis. Cardiology Clinics. 1993;11(4):603–616. - PubMed
-
- Perloff JK. Survival patterns without cardiac surgery or interventional catheterization: a narrowing base. In: Perloff JK, Childs JS, editors. Congenital Heart Disease in Adults. 2nd edition. Philadelphia, Pa, USA: WB Saunders; 1998. pp. 15–53.
-
- Guleserian KJ. Adult congenital heart disease: surgical advances and options. Progress in Cardiovascular Diseases. 2011;53(4):254–264. - PubMed
-
- Tucker WR, Davies DC, Anderson RH, Lagolopulos M, Webb S. Muscular ventricular septal defect in an 89-year-old woman that was undetected during life. Clinical Anatomy. 2003;16(6):522–525. - PubMed
LinkOut - more resources
Full Text Sources
