

Review
doi: 10.2174/1573403x10666140514103309.
Current algorithms for the diagnosis of wide QRS complex tachycardias
Affiliations
- PMID: 24827795
- PMCID: PMC4040878
- DOI: 10.2174/1573403x10666140514103309
Item in Clipboard
Review
Current algorithms for the diagnosis of wide QRS complex tachycardias
Curr Cardiol Rev.
2014 Aug.
Abstract
The differential diagnosis of a regular, monomorphic wide QRS complex tachycardia (WCT) mechanism represents a great diagnostic dilemma commonly encountered by the practicing physician, which has important implications for acute arrhythmia management, further work-up, prognosis and chronic management as well. This comprehensive review discusses the causes and differential diagnosis of WCT, and since the ECG remains the cornerstone of WCT differential diagnosis, focuses on the application and diagnostic value of different ECG criteria and algorithms in this setting and also provides a practical clinical approach to patients with WCTs.
Figures

Recognition of AV dissociation using the Lewis leads. The upper panel shows a WCT due to VT in a patient with recurrent monomorphic VTs. Although the suspicion of AV dissociation might emerge looking at the standard 12 lead ECG, the P waves cannot be discerned with certainty. The lower panel shows a somewhat later recorded rhythm strip with the Lewis lead, which should be interpreted in lead I, while the patient was on amiodarone treatment. The vertical black arrows indicate dissociated P waves (courtesy of András Simon MD). For further explanation see text.

The Brugada algorithm. For further explanation see text.

An example of a WCT due to SVT
demonstrating why the presence of an initial R wave in lead aVR
criterion might be superior to the traditional northwest axis
criterion. The QRS axis is -160o, northwest axis
suggesting the misdiagnosis of VT. Although the QRS complex is
predominantly positive in lead aVR, there is no initial R wave,
because the QRS complex starts with a q wave, and the vi/vt
in lead aVR >1, suggesting correctly SVT. Reproduced from Ref. 18.
with permission.
The first Vereckei algorithm. FB=fascicular block. For further explanation see text.

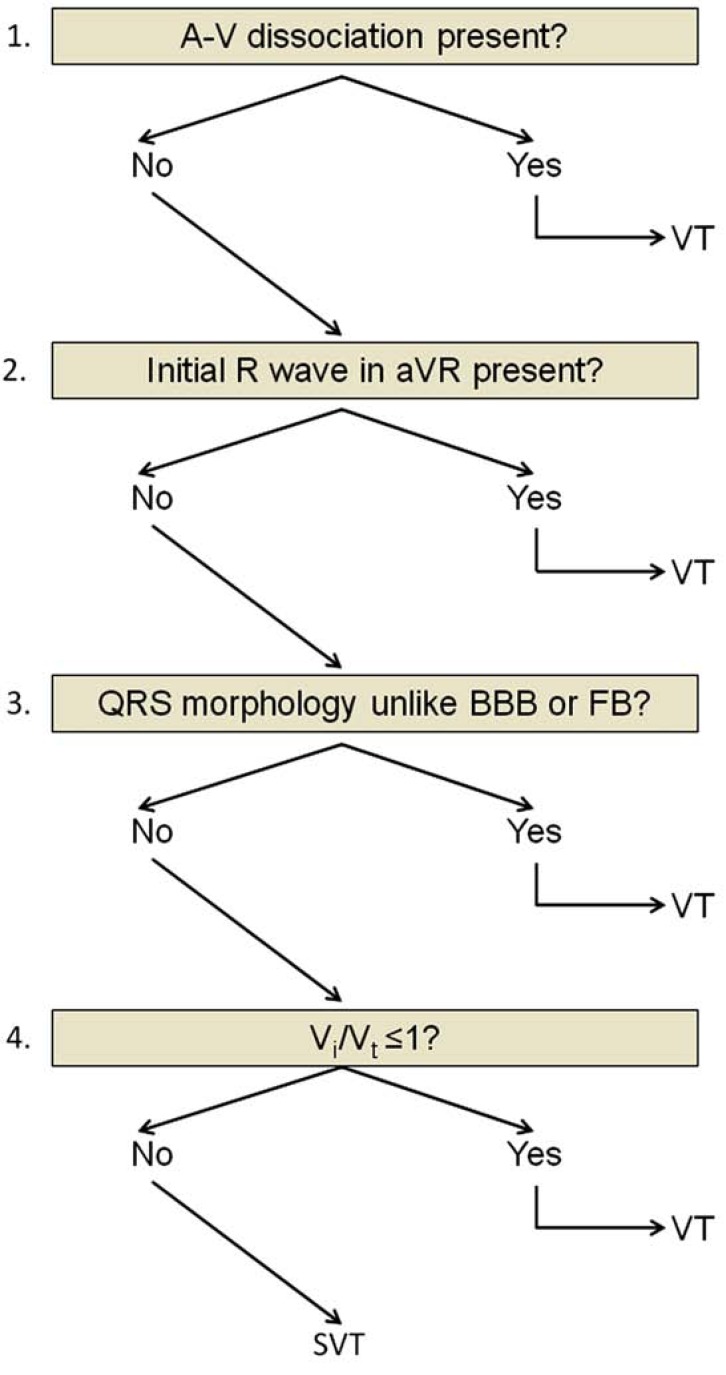
The aVR Vereckei algorithm. For further explanation see text.
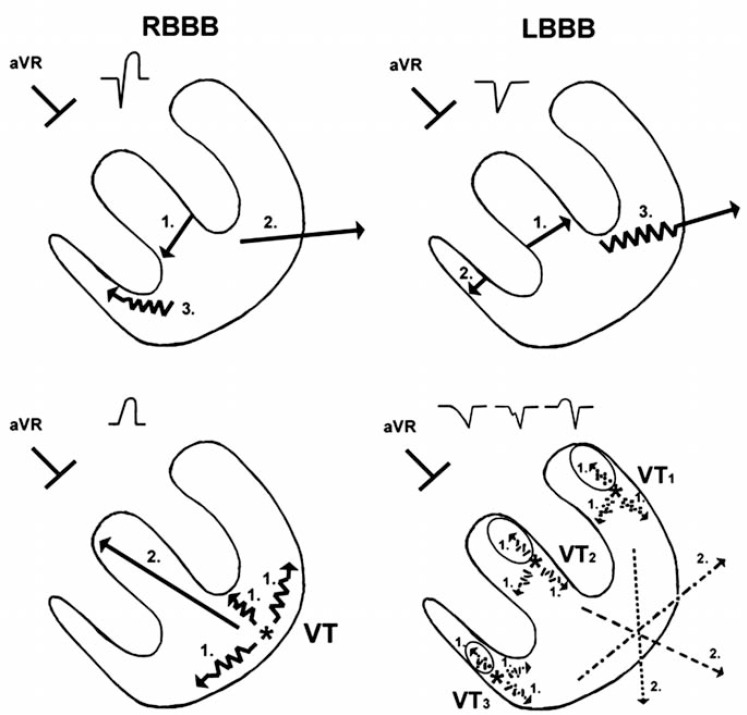
Schematic explanation of the rationale behind the aVR Vereckei algorithm criteria. The vectors marked with serrated lines and number 1 in the two lower panels are representing the slow initial upward vector components pointing toward lead aVR, which are present in all VTs regardless of the site of origin. The vectors marked with number 2 in the two lower panels represent the resultant QRS vectors of ventricular activation. For further explanation see text.

Representative examples of the most common lead aVR ECG patterns taken from real tracings recorded from patients with WCTs superimposed on a grid (small box=40 ms). For further explanation see text. Reproduced from Ref. 19. with permission.

The algorithm of Brugada working group devised for distinguishing VT from PXT. For further explanation see text.

The algorithm proposed by the ACC/AHA/ESC guideline for WCT differential diagnosis.
References
-
- Miller JM, Das MK, editors. In: Cardiac electrophysiology. From cell to bedside. 5th Edition. Eds. Elsevier.: Zipe DPJalife J. Saunders.; 2009. Differential diagnosis for wide QRS complex tachycardia. pp. 823–30.
-
- Issa F, Miller JM, Zipes DP, editors. Approach to wide QRS complex tachycardias. 2nd Edition. Elsevier Saunders: 2012. Clinical arrhythmology and electrophysiology. pp. 499–511.
-
- Pellegrini CN, Scheinman MM. Clinical management of ventricular tachycardia. Curr Probl Cardiol. 2010;35:453–504. - PubMed
-
- Alzand BSN, Crijns HJGM. Diagnostic criteria of broad QRS complex tachycardia: decades of evolution. Europace. 2011;13:465–72. - PubMed
-
- Benito B, Josephson ME. Ventricular tachycardia in coronary artery disease. Revista Espanola de Cardiologia. 2012;65:939–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
