

Electrocardiogram in Andersen-Tawil syndrome. New electrocardiographic criteria for diagnosis of type-1 Andersen-Tawil syndrome
- PMID: 24827800
- PMCID: PMC4040873
- DOI: 10.2174/1573403x10666140514102528
Electrocardiogram in Andersen-Tawil syndrome. New electrocardiographic criteria for diagnosis of type-1 Andersen-Tawil syndrome
Abstract
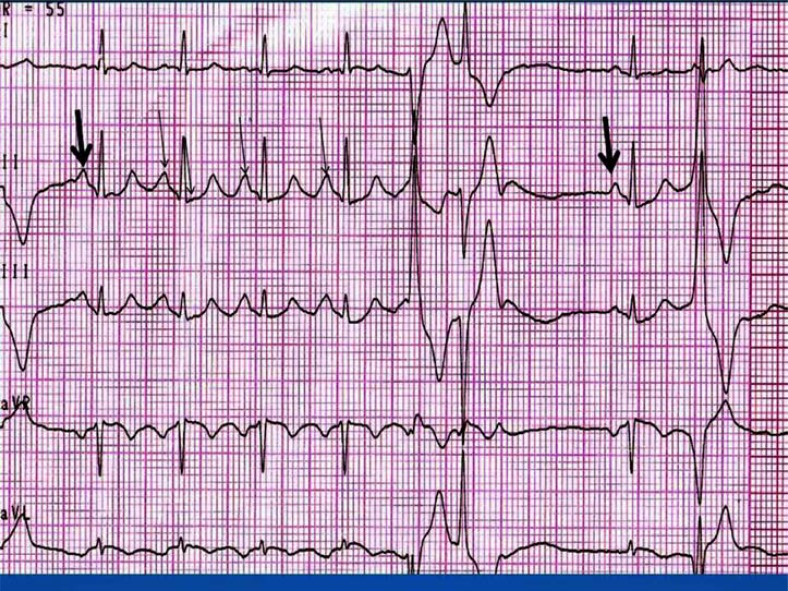
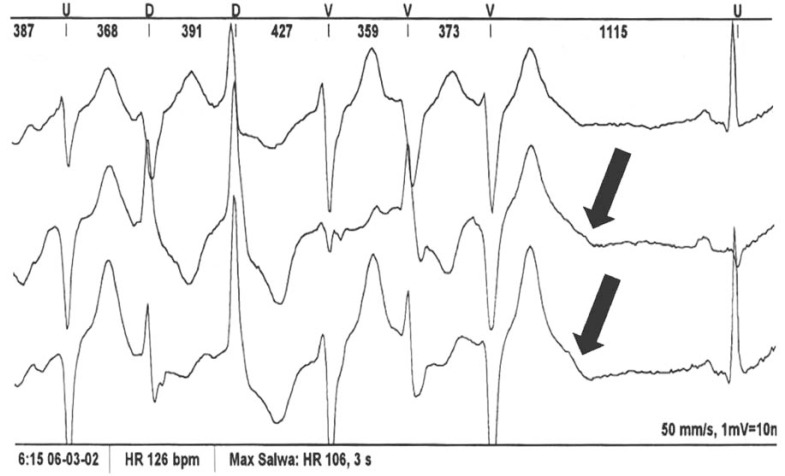
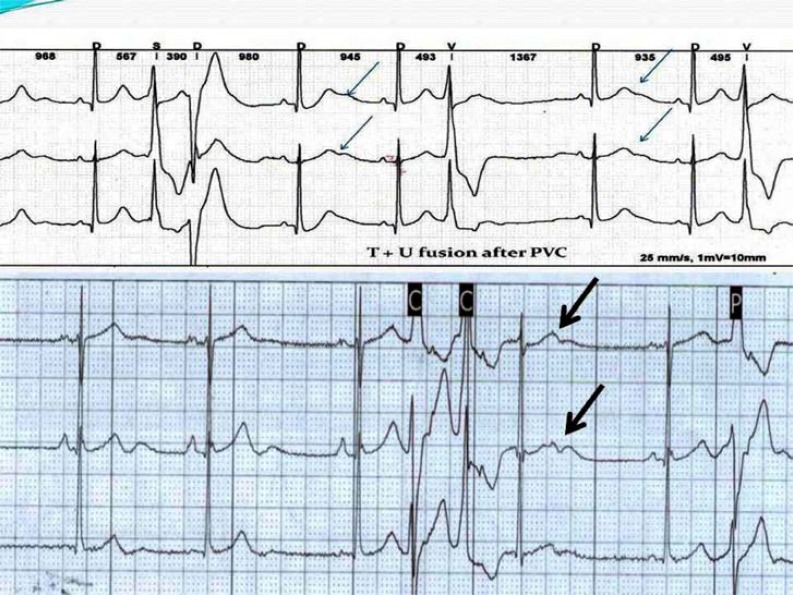
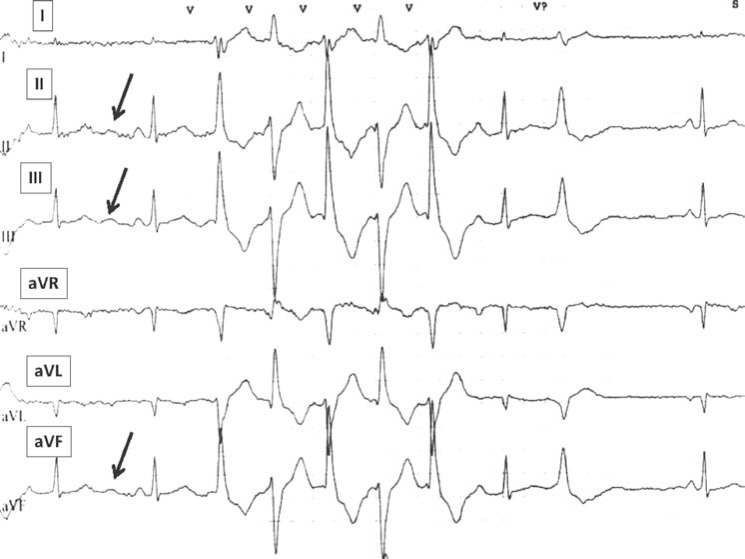
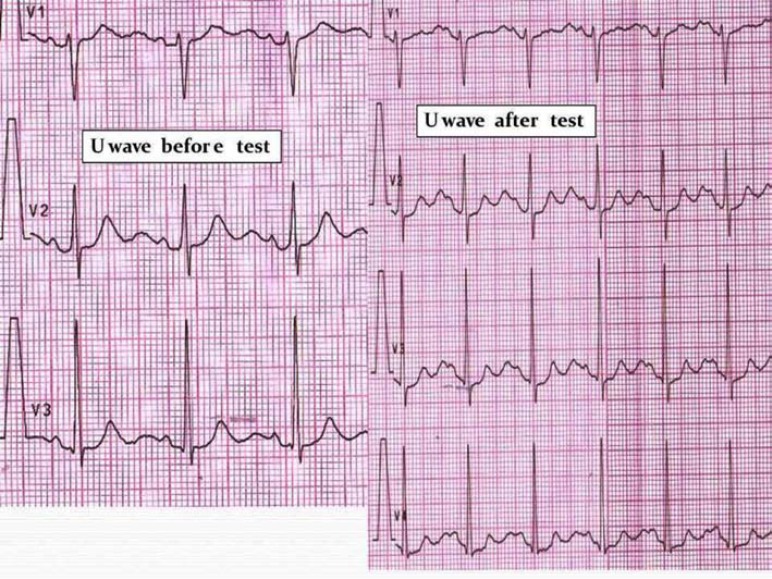
Andersen - Tawil syndrome (ATS) is an autosomal - dominant or sporadic disorder characterized by ventricular arrhythmias, periodic paralysis, and distinctive facial and skeletal dysmorphism. Mutations in KCNJ2, which encodes the α-subunit of the potassium channel Kir2.1, were identified in patients with ATS. This genotype has been designated as type-1 ATS (ATS1). KCNJ2 mutations are detectable in up to 60 % of patients with ATS. Cardiac manifestations of ATS include frequent premature ventricular contractions (PVC), Q-U interval prolongation, prominent U-waves, and a special type of polymorphic ventricular tachycardia (PMVT) called bidirectional ventricular tachycardia (BiVT). The presence of frequent PVCs at rest are helpful in distinguishing ATS from typical catecholaminergic polymorphic ventricular tachycardia (CPVT). In typical CPVT, rapid PMVT and BiVT usually manifest during or after exercising. Additionally, CPVT or torsade de pointes in LQTS are faster, very symptomatic causing syncope or often deteriorate into VF resulting in sudden cardiac death. PVCs at rest are quite frequent in ATS1 patients, however, in LQTS patients, PVCs and asymptomatic VT are uncommon which also contributes to differentiating them. The article describes the new electrocardiographic criteria proposed for diagnosis of type-1 Andersen-Tawil syndrome. A differential diagnosis between Andersen-Tawil syndrome, the catecholamine polymorphic ventiruclar tachycardia and long QT syndrome is depicted. Special attention is paid on the repolarization abnormalities, QT interval and the pathologic U wave. In this article, we aim to provide five new electrocardiographic clues for the diagnosis of ATS1.
Figures
References
-
- Andersen E, Krasilnikoff PA, Overvad H. Intermittent muscular weakness. extrasystles.and multiple developmental anomalies new syndrome?. . Acta Pediatric Scan. 1971;60: 559–64. - PubMed
-
- Tawil R, Ptacek LJ, Pavlakis SG , et al. Andersen`s syndrome: potassium-sensitive periodic paralysis. ventricular ecopy.and dysmorphic features. Ann Neurol . 1994; 35:326–30. - PubMed
-
- Donaldson MR, Yoon G, Fu YH, Ptacek LJ. Andersen-Tawil syndrome: a model of clinical variability. pleiotopy.and genetic heterogeneity. Ann Med . 2004; 36 (Suppl 1 ):92–7. - PubMed
-
- Plaster NM, Tawil R, Tristani-Firouzi M , et al. Mutations in Kir..1 cause the developmental and episodic electrical phenotypes of Andresen`s syndrome. Cell. 2001;105:511–9. - PubMed
-
- Hosaka Y, Hanawa H, Washizuka T , et al. Function. subcellular localization and assembly of a novel mutation of KCNJ2 in Andersen’s syndrome. J Mol Cell Cardiol. 2003;35:409–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
