

Increased arterial inflammation relates to high-risk coronary plaque morphology in HIV-infected patients
- PMID: 24828267
- PMCID: PMC4023912
- DOI: 10.1097/QAI.0000000000000138
Increased arterial inflammation relates to high-risk coronary plaque morphology in HIV-infected patients
Abstract
Background: Mechanisms predisposing HIV-infected patients to increased cardiovascular disease (CVD) risk remain unclear.
Objective: To determine the interrelationship between arterial inflammation and high-risk coronary plaque morphology in HIV-infected patients with subclinical coronary atherosclerosis.
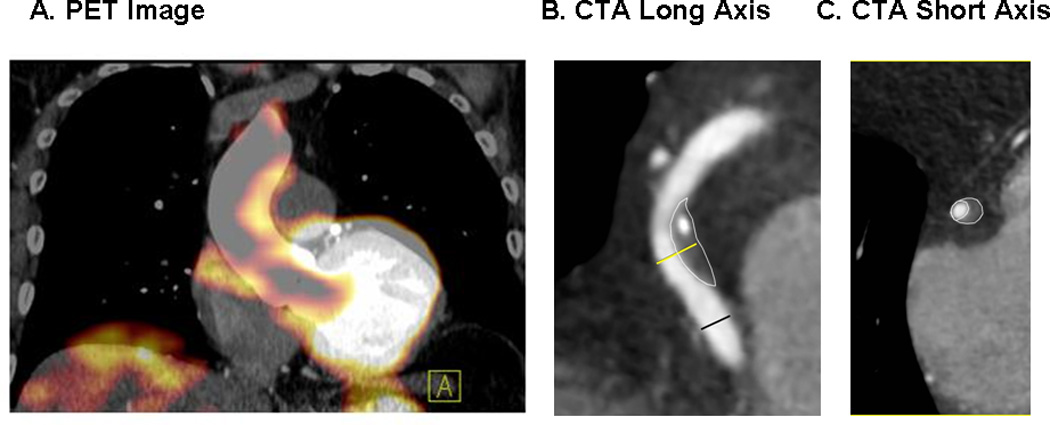
Methods: Forty-one HIV-infected patients on stable antiretroviral therapy without known CVD but with atherosclerotic plaque on coronary CT angiography were evaluated with F-FDG-PET. Patients were stratified into 2 groups based on relative degree of arterial inflammation [aortic target-to-background ratio (TBR)]. High-risk coronary atherosclerotic plaque morphology features were compared between groups.
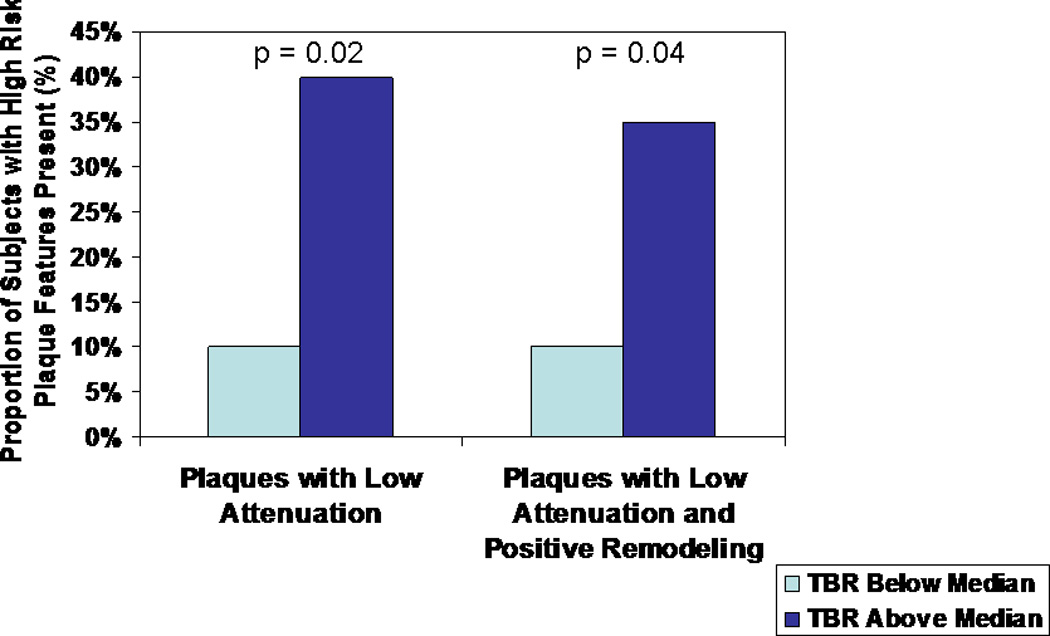
Results: HIV-infected patients with higher and lower TBRs were similar with respect to traditional CVD risk parameters. Among HIV-infected patients with higher TBR, an increased percentage of patients demonstrated at least 1 low-attenuation coronary atherosclerotic plaque (40% vs. 10%, P = 0.02) and at least 1 coronary atherosclerotic plaque with both low attenuation and positive remodeling (35% vs. 10%, P = 0.04). Moreover, in the higher TBR group, both the number of low-attenuation plaques per patient (P = 0.02) and the number of vulnerability features in the most vulnerable plaque (P = 0.02) were increased. TBR grouping remained significantly related to the number of low-attenuation plaques/subject (β = 0.35, P = 0.004), controlling for age, gender, low-density lipoprotein, duration of HIV, and CD4.
Conclusions: These data demonstrate a relationship between arterial inflammation on F-FDG-PET and high-risk coronary atherosclerotic plaque features among HIV-infected patients with subclinical coronary atherosclerosis. Further studies are needed to determine whether arterial inflammation and related high-risk coronary morphology increase the risk of clinical CVD events in the HIV population.
Figures
References
-
- Baker J, Hullsiek KH, Singh A, et al. CROI. Atlanta, GA: 2013. Monocyte Activation, but not T cell Activation, Predicts Progression of Coronary Artery Calcium in a Contemporary HIV Cohort; p. 66. LB.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
