

Management of acute right ventricular failure in the intensive care unit
- PMID: 24828526
- PMCID: PMC4225807
- DOI: 10.1513/AnnalsATS.201312-446FR
Management of acute right ventricular failure in the intensive care unit
Abstract
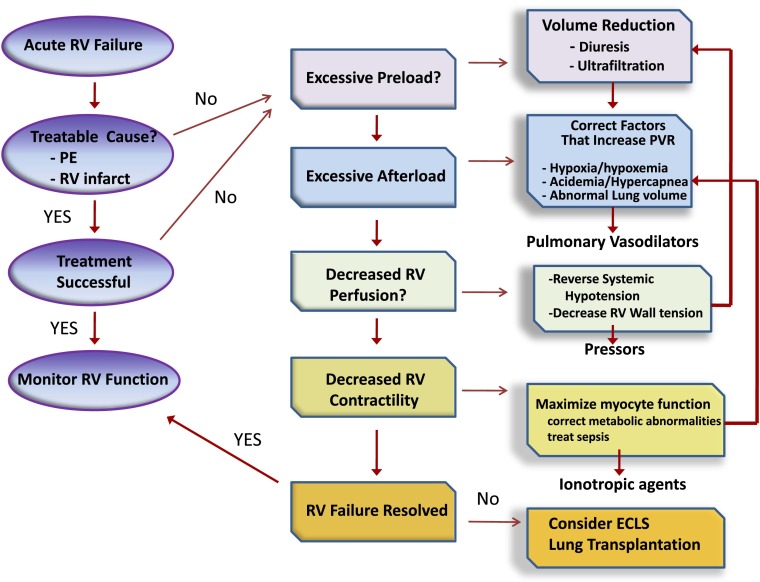
Right ventricular (RV) failure occurs when the RV fails to maintain enough blood flow through the pulmonary circulation to achieve adequate left ventricular filling. This can occur suddenly in a previously healthy heart due to massive pulmonary embolism or right-sided myocardial infarction, but many cases encountered in the intensive care unit involve worsening of compensated RV failure in the setting of chronic heart and lung disease. Management of RV failure is directed at optimizing right-sided filling pressures and reducing afterload. Due to a lower level of vascular tone, vasoactive medications have less salient effects on reducing vascular resistance in the pulmonary than in the systemic circulation. Successful management requires reversal of any conditions that heighten pulmonary vascular tone and the use of selective pulmonary vasodilators at doses that do not induce systemic hypotension or worsening of oxygenation. Systemic systolic arterial pressure should be kept close to RV systolic pressure to maintain RV perfusion. When these efforts fail, the judicious use of inotropic agents may help improve RV contractility enough to maintain cardiac output. Extracorporeal life support is increasingly being used to support patients with acute RV failure who fail to respond to medical management while the underlying cause of their RV failure is addressed.
Keywords: critical care; pulmonary hypertension; right-sided heart failure.
Figures



References
-
- Bhattacharya J, Staub NC. Direct measurement of microvascular pressures in the isolated perfused dog lung. Science. 1980;210:327–328. - PubMed
-
- Dell’Italia LJ. The right ventricle: anatomy, physiology, and clinical importance. Curr Probl Cardiol. 1991;16:653–720. - PubMed
-
- Greyson CR. Pathophysiology of right ventricular failure. Crit Care Med. 2008;36(1) Suppl:S57–S65. - PubMed
-
- James TN. Anatomy of the crista supraventricularis: its importance for understanding right ventricular function, right ventricular infarction and related conditions. J Am Coll Cardiol. 1985;6:1083–1095. - PubMed
-
- Pouleur H, Lefèvre J, Van Mechelen H, Charlier AA. Free-wall shortening and relaxation during ejection in the canine right ventricle. Am J Physiol. 1980;239:H601–H613. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
